Arnljots Rebeka, Thorn Jörgen, Elm Marie, Moore Michael, Sundvall Pär-Daniel
Närhälsan, Research and Development Primary Health Care, Region Västra Götaland, Research and Development Center Södra Älvsborg Sweden, Sven Eriksonsplatsen 4, SE-503 38, Borås, Sweden.
Department of Public Health and Community Medicine/Primary Health Care, Institute of Medicine, Sahlgrenska Academy at the University of Gothenburg, Box 454, SE-405 30, Gothenburg, Sweden.
BMC Geriatr. 2017 Oct 10;17(1):229. doi: 10.1186/s12877-017-0622-1.
Residents of nursing homes may have low 25-hydroxyvitamin D (25OHD) concentrations. Associations between vitamin D and cognitive performance, dementia and susceptibility to infections are not clearly established. The aim of this study was to investigate the prevalence of vitamin D deficiency and to identify associated factors among residents of nursing homes for elderly.
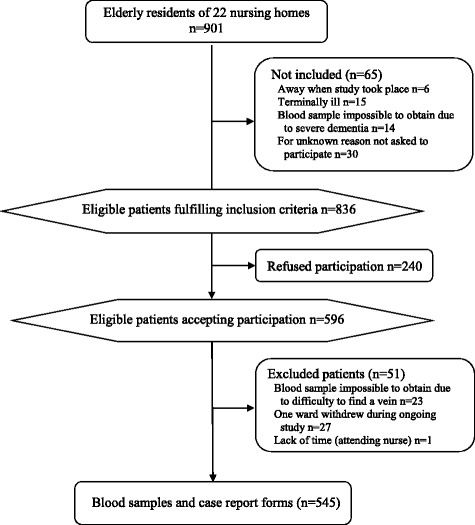
In this cross-sectional study blood samples for analysis of 25OHD were collected from all participating residents of Swedish nursing homes for the elderly from January to March 2012.
dementia too severe to collect a blood test, terminally ill or refusing participation.
Serum 25OHD concentrations. Logistic regression to evaluate factors associated with vitamin D deficiency (25OHD < 25 nmol/L).
Blood samples were obtained from 545 of 901 residents of 22 nursing homes. Mean age 86 years (SD 6.9), 68% were women. Prevalence of vitamin D supplementation 17%, dementia 55%, lack of appetite ≥3 months 45% and any antibiotic treatment during the last 6 months 30%. Serum 25OHD concentrations: mean 34 nmol/L (SD 21, median 27, range 4-125), 82% (448/545) had 25OHD < 50 nmol/L and 41% (224/545) had 25OHD < 25 nmol/L. Adjusted OR (95% CI; p-value) for possible predictors of vitamin D deficiency (25OHD < 25 nmol/L): vitamin D supplementation 0.075 (0.031-0.18; p < 0.001), lack of appetite ≥3 months 0.75 (0.50-1.1; p = 0.15), hours outdoors/week 0.99 (0.96-1.0; p = 0.62), Fitzpatrick skin phototype (4-6) 0.69 (0.44-1.1; p = 0.12); dementia 2.3 (1.5-3.4; p < 0.001) and antibiotics last 6 months 1.6 (1.1-2.6; p < 0.029), adjusted for age and gender.
Vitamin D deficiency was common among nursing home residents and strongly associated with dementia. Regardless of causality or not, it is important to be alert for vitamin D deficiency in nursing homes residents with dementia. As expected vitamin D supplementation was associated with less vitamin D deficiency, however lack of appetite, staying outdoors and skin phototype were not significant predictors. Antibiotic treatments during the last 6 months were associated with vitamin D deficiency, potentially supporting the hypothesis that vitamin D deficiency is associated with infections.
疗养院居民的25-羟基维生素D(25OHD)浓度可能较低。维生素D与认知能力、痴呆症和感染易感性之间的关联尚未明确确立。本研究的目的是调查维生素D缺乏症的患病率,并确定老年疗养院居民中的相关因素。
在这项横断面研究中,于2012年1月至3月从瑞典老年疗养院的所有参与居民中采集用于分析25OHD的血样。
痴呆严重到无法进行血液检测、晚期疾病或拒绝参与。
血清25OHD浓度。采用逻辑回归评估与维生素D缺乏(25OHD < 25 nmol/L)相关的因素。
从22家疗养院的901名居民中获取了545份血样。平均年龄86岁(标准差6.9),68%为女性。维生素D补充剂的使用率为17%,痴呆症患病率为55%,食欲缺乏≥3个月的比例为45%,过去6个月内接受过任何抗生素治疗的比例为30%。血清25OHD浓度:平均值为34 nmol/L(标准差21,中位数27,范围4 - 125),82%(448/545)的25OHD < 50 nmol/L,41%(224/545)的25OHD < 25 nmol/L。维生素D缺乏(25OHD < 25 nmol/L)可能预测因素的校正比值比(95%置信区间;p值):维生素D补充剂0.075(0.031 - 0.18;p < 0.001),食欲缺乏≥3个月0.75(0.50 - 1.1;p = 0.15),每周户外活动小时数0.99(0.96 - 1.0;p = 0.62),菲茨帕特里克皮肤光类型(4 - 6)0.69(0.44 - 1.1;p = 0.12);痴呆症2.3(1.5 - 3.4;p < 0.001)以及过去6个月内使用抗生素1.6(1.1 - 2.6;p < 0.029),校正了年龄和性别因素。
维生素D缺乏在疗养院居民中很常见,且与痴呆症密切相关。无论因果关系如何,对患有痴呆症的疗养院居民的维生素D缺乏情况保持警惕很重要。正如预期的那样,维生素D补充剂与较少的维生素D缺乏相关,然而食欲缺乏、户外活动时间和皮肤光类型并非显著的预测因素。过去6个月内的抗生素治疗与维生素D缺乏相关,这可能支持维生素D缺乏与感染相关的假说。