Yamagata Toru, Naito Kentaro, Yoshimura Masaki, Ohata Kenji, Takami Toshihiro
Department of Neurosurgery, Osaka City General Hospital, Osaka, Japan.
Department of Neurosurgery, Osaka City University Graduate School of Medicine, Osaka, Japan.
J Craniovertebr Junction Spine. 2017 Jul-Sep;8(3):179-186. doi: 10.4103/jcvjs.JCVJS_57_17.
Postoperative oropharyngeal complications such as dysphagia after anterior cervical spine surgery are some of the least discussed surgery-related complications. The purpose of this retrospective study is to investigate the incidence and possible risk factors for 30-day postoperative dysphagia after anterior cervical discectomy and fusion (ACDF).
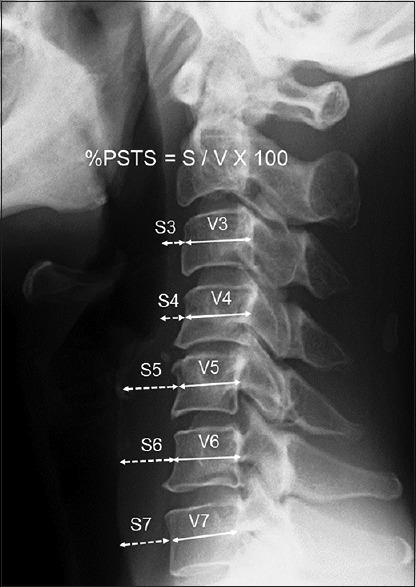
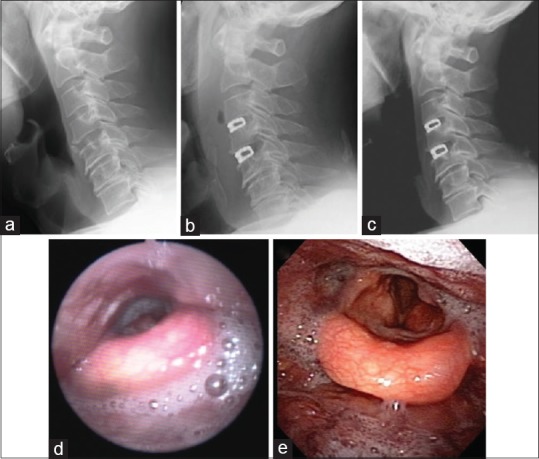
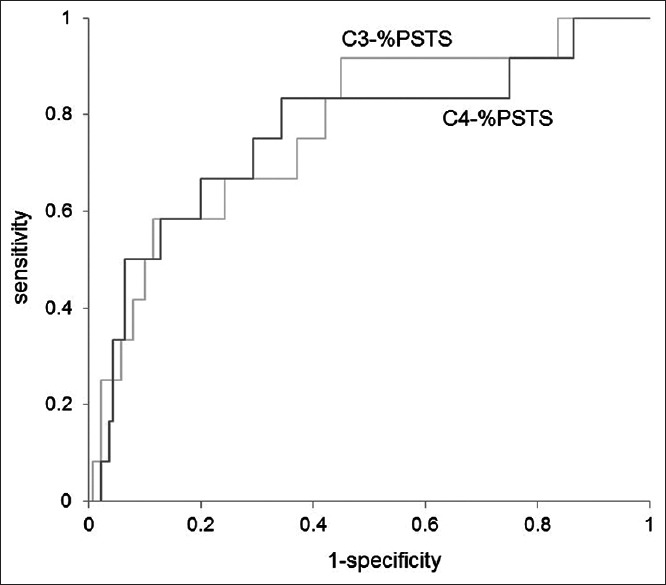
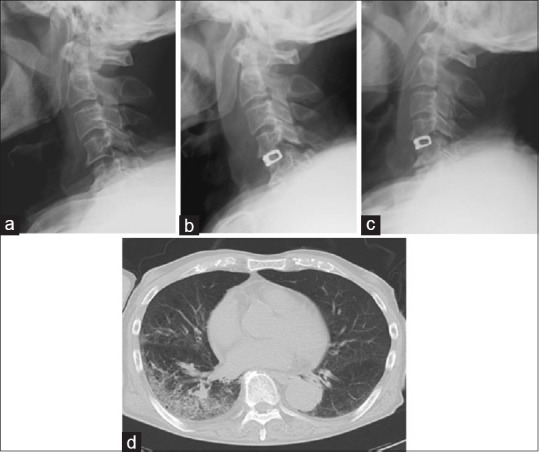
This study included 152 consecutive patients who underwent 1- or 2-level ACDF using a rectangular titanium stand-alone cage in our institutes. Surgery-related dysphagia early after surgery was analyzed based on hospital charts. Radiological evaluation of prevertebral soft tissue swelling (PSTS) was performed by comparing plain lateral radiographs of the cervical spine before surgery with those after surgery. The percentage of PSTS (%PSTS) was defined by retropharyngeal soft tissue diameter divided by vertebral diameter. Positive %PSTS was determined when %PSTS exceeded its mean + 2 standard deviations.
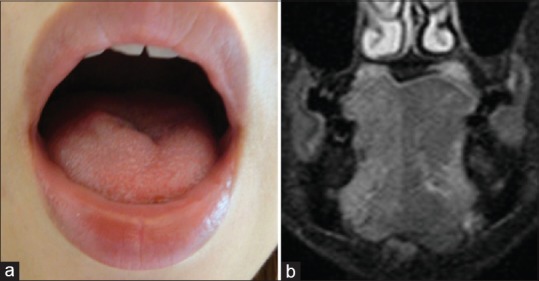
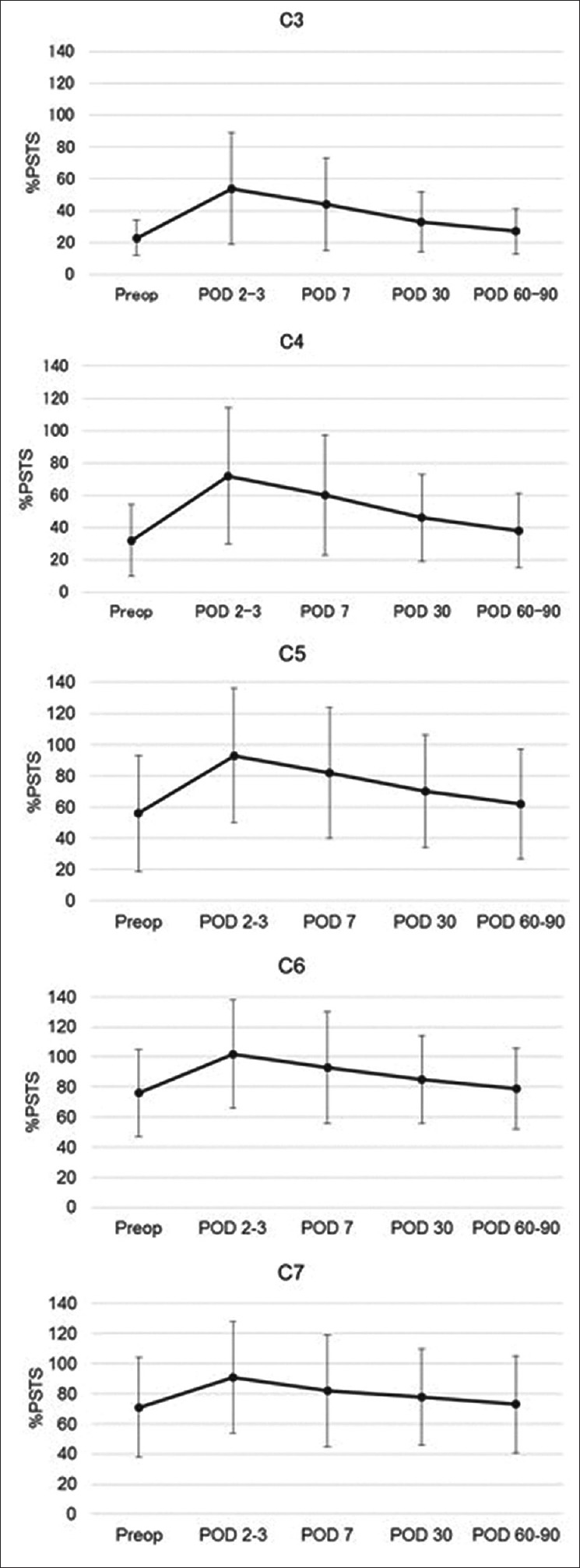
Twelve patients (7.9%) demonstrated prolonged symptoms of dysphagia within 30-day postoperatively. All patients eventually demonstrated satisfactory or acceptable recovery late after surgery, except one case of hypoglossal nerve palsy. %PSTS was significantly highest early after surgery and returned to presurgical levels within 30 days after surgery. Statistical analysis suggested that the positive %PSTS at C3 or C4 level early after surgery was significantly associated with the occurrence of postoperative dysphagia.
Although the possible reasons for postoperative dysphagia may not only be multifactorial but also be highly surgeon-dependent, such a complication is still underestimated and needs to be carefully resolved. %PSTS appeared to be easy and reliable index to judge the possible risk of postoperative dysphagia.
颈椎前路手术后的口咽并发症,如吞咽困难,是最少被讨论的手术相关并发症之一。本回顾性研究的目的是调查颈椎前路椎间盘切除融合术(ACDF)术后30天吞咽困难的发生率及可能的危险因素。
本研究纳入了我院152例连续接受单节段或双节段ACDF并使用矩形钛独立椎间融合器的患者。根据医院病历分析术后早期与手术相关的吞咽困难情况。通过比较术前和术后颈椎侧位平片对椎前软组织肿胀(PSTS)进行影像学评估。PSTS百分比(%PSTS)定义为咽后软组织直径除以椎体直径。当%PSTS超过其均值加2个标准差时判定为%PSTS阳性。
12例患者(7.9%)术后30天内出现吞咽困难症状延长。除1例舌下神经麻痹外,所有患者术后晚期最终均显示出满意或可接受的恢复情况。%PSTS在术后早期显著最高,并在术后30天内恢复到术前水平。统计分析表明,术后早期C3或C4水平的%PSTS阳性与术后吞咽困难的发生显著相关。
尽管术后吞咽困难的可能原因可能不仅是多因素的,而且高度依赖外科医生,但这种并发症仍被低估,需要仔细解决。%PSTS似乎是判断术后吞咽困难可能风险的简单可靠指标。