Hasturk Askin Esen, Gokce Emre Cemal, Elbir Cagri, Gel Gulce, Canbay Suat
Department of Neurosurgery, Oncology Education and Research Hospital, Ankara, Turkey.
J Craniovertebr Junction Spine. 2017 Jul-Sep;8(3):253-262. doi: 10.4103/jcvjs.JCVJS_1_17.
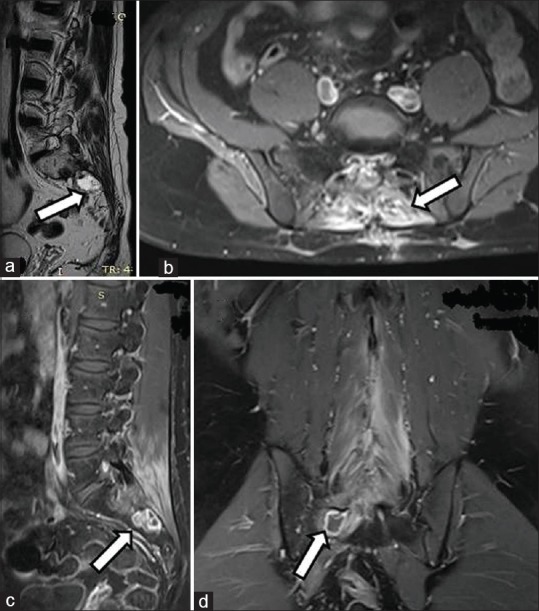
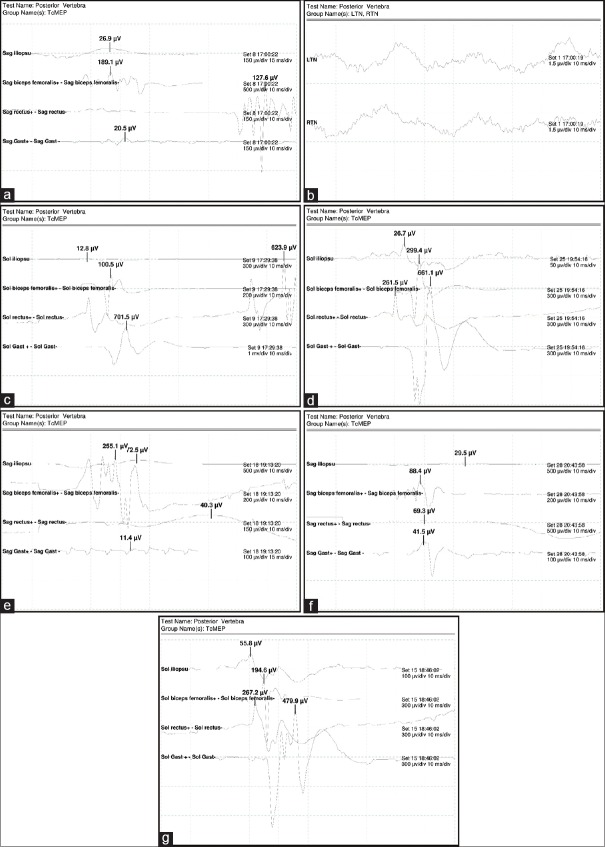
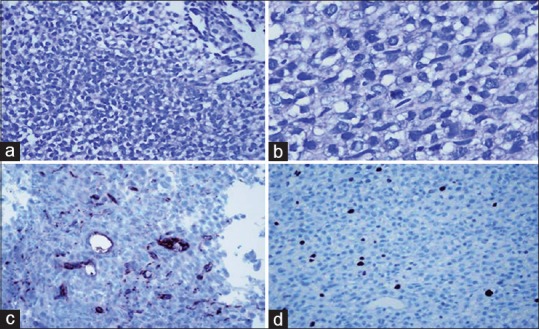
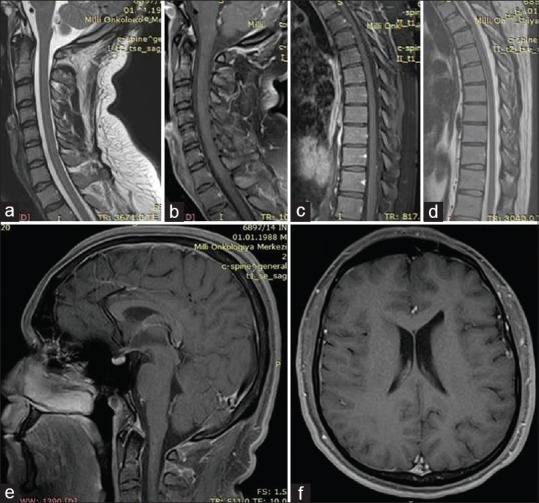
In this study, we evaluated a case of primary spinal oligodendroglioma (PSO) with a rare localization between L3 and S2, and also examined sixty cases in the literature in terms of demographic characteristics, clinical, radiological, and histopathological characteristics, and treatment planning. A case of PSO has been presented, and the relevant literature between 1931 and 2016 was reviewed. A total of 57 papers regarding PSO were found and utilized in this review. The main treatment options include radical surgical excision with neuromonitoring, followed by radiotherapy. Despite these treatment protocols, the relapse rate is high, and treatment does not significantly prolong survival. Oligodendrogliomas are rare among the primary spinal cord tumors. Oligodendrogliomas are predominantly found in the cervical spinal cord, thoracic spinal cord, or junctions during childhood and adulthood. Extension to the sacral region, inferior to the Conus, is very rare. Furthermore, of the sixty cases in the literature, the case we present here is the first to be reported in this particular age group. These localizations usually occur in the pediatric age group and after relapses. While for a limited number of cases the oligodendroglioma initiates in the thoracic region and reaches as far as L2, we encountered a case of an oligodendroglioma within the range of L3 to S2. Clinical findings are observed in accordance with location, and magnetic resonance imaging is the gold standard for diagnosis.
在本研究中,我们评估了一例原发性脊髓少突胶质细胞瘤(PSO),其位于L3和S2之间,位置罕见,并且还从人口统计学特征、临床、放射学和组织病理学特征以及治疗规划方面对文献中的60例病例进行了研究。本文报告了一例PSO病例,并回顾了1931年至2016年间的相关文献。本综述共检索并使用了57篇关于PSO的论文。主要治疗选择包括在神经监测下进行根治性手术切除,随后进行放疗。尽管有这些治疗方案,但复发率很高,且治疗并不能显著延长生存期。少突胶质细胞瘤在原发性脊髓肿瘤中较为罕见。少突胶质细胞瘤主要见于儿童期和成年期的颈髓、胸髓或其交界处。延伸至骶骨区域、圆锥以下的情况非常罕见。此外,在文献中的60例病例中,我们这里报告的病例是该特定年龄组中首例报告的病例。这些定位通常发生在儿童年龄组以及复发后。虽然少数情况下少突胶质细胞瘤起源于胸段并延伸至L2,但我们遇到了一例位于L3至S2范围内的少突胶质细胞瘤。临床症状根据位置出现,磁共振成像(MRI)是诊断的金标准。