Yu Ho Song, Hwang Jun Eul, Chung Ho Seok, Cho Yang Hyun, Kim Myung Soo, Hwang Eu Chang, Oh Kyung Jin, Kim Sun-Ouck, Jung Seung Il, Kang Taek Won, Kwon Dong Deuk, Park Kwangsung, Ryu Soo Bang, Jung Sung-Hoon, Hur Young Hoe, Noh Joon Hwa, Kim Myung Ki, Seo Ill Young, Kim Chul-Sung, Kang Sung Gu, Kang Seok Ho, Cheon Jun
Department of Urology, Chonnam National University Medical School, Gwangju, Korea.
Department of Hemato-Oncology, Chonnam National University Medical School, Gwangju, Korea.
Oncotarget. 2017 Mar 15;8(39):66540-66549. doi: 10.18632/oncotarget.16239. eCollection 2017 Sep 12.
The aim of this study was to determine the effect of preoperative chronic kidney disease (CKD) on the prognosis of patients with upper urinary tract urothelial carcinoma (UTUC) who had undergone radical nephroureterectomy (RNU).
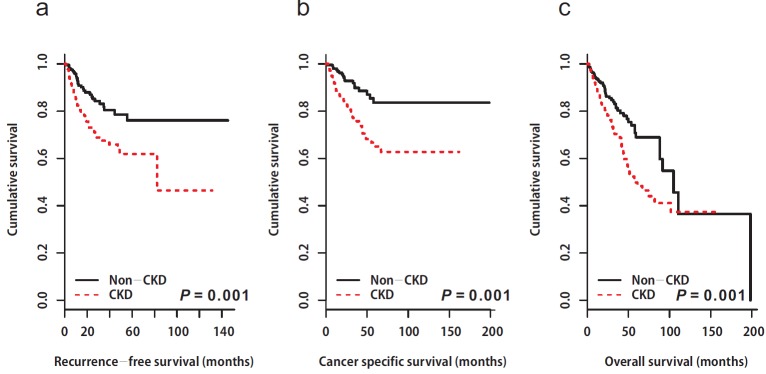
The median follow-up period was 31.1 months (interquartile range: 16.2-55.7 months). Among the study patients, 224 patients in the non-CKD group were selected propensity score matching. The median recurrence-free, cancer-specific, and overall survival were significantly shorter for patients with preoperative CKD than for non-CKD patients ( = 0.001, = 0.001, and = 0.001, respectively). According to multivariable Cox regression analysis, preoperative CKD was related to worse recurrence-free (hazard ratio [HR]: 1.81, 95% confidence interval [CI]: 1.15-2.86, = 0.011), cancer-specific (HR: 2.44, 95% CI: 1.44-4.14, = 0.001), and overall survival (HR: 1.66, 95% CI: 1.15-2.40, = 0.007).
A total of 566 patients who underwent RNU at 6 institutions from 2004 to 2014 were retrospectively reviewed. Of these patients, 342 had an estimated glomerular filtration rate (eGFR) ≥ 60 ml/min/1.73 m (non-CKD group) and 224 patients had an eGFR <60 ml/min/1.73 m (CKD group). To adjust for potential baseline confounders, 224 patients in the non-CKD group were selected by propensity matching. Clinicopathological variables and survival rates were compared between the 2 groups.
Preoperative CKD appears to be an important independent prognostic factor for oncologic outcomes in patients with UTUC.
本研究旨在确定术前慢性肾病(CKD)对接受根治性肾输尿管切除术(RNU)的上尿路尿路上皮癌(UTUC)患者预后的影响。
中位随访期为31.1个月(四分位间距:16.2 - 55.7个月)。在研究患者中,非CKD组的224例患者通过倾向评分匹配进行选择。术前患有CKD的患者的无复发生存期、癌症特异性生存期和总生存期的中位数显著短于非CKD患者(分别为P = 0.001、P = 0.001和P = 0.001)。根据多变量Cox回归分析,术前CKD与较差的无复发生存期(风险比[HR]:1.81,95%置信区间[CI]:1.15 - 2.86,P = 0.011)、癌症特异性生存期(HR:2.44,95%CI:1.44 - 4.14,P = 0.001)和总生存期(HR:1.66,95%CI:1.15 - 2.40,P = 0.007)相关。
回顾性分析了2004年至2014年在6家机构接受RNU的566例患者。其中,342例患者的估计肾小球滤过率(eGFR)≥60 ml/min/1.73㎡(非CKD组),224例患者的eGFR <60 ml/min/1.73㎡(CKD组)。为了调整潜在的基线混杂因素,通过倾向匹配从非CKD组中选择了224例患者。比较了两组的临床病理变量和生存率。
术前CKD似乎是UTUC患者肿瘤学结局的重要独立预后因素。