Center for Tobacco Control Research and Education, and Department of Medicine, University of California, San Francisco, San Francisco, California.
Center for Tobacco Control Research and Education, and Department of Medicine, University of California, San Francisco, San Francisco, California.
Am J Prev Med. 2017 Dec;53(6):810-817. doi: 10.1016/j.amepre.2017.08.004. Epub 2017 Oct 10.
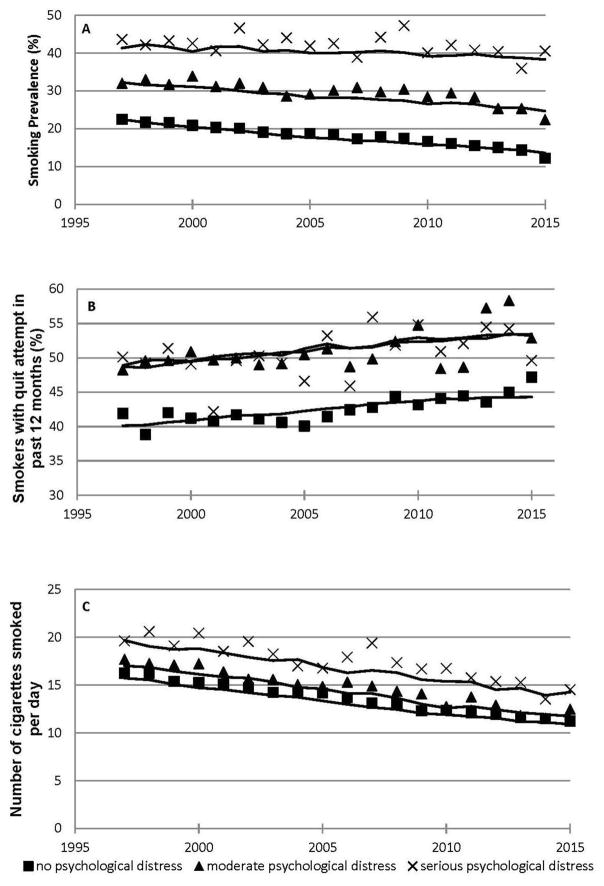
It has been argued that as smoking prevalence declines, the remaining smokers represent a "hard core" who are unwilling or unable to quit, a process known as hardening. However, as recently shown, the general smoking population is softening not hardening (i.e., as prevalence falls, more quit attempts and lower consumption among continuing smokers). People with psychological distress smoke more, so they may represent hard-core smokers.
Using cross-sectional time series analysis, in 2016-2017 changes in quit attempts and cigarette consumption were evaluated over 19 years among smokers with serious psychological distress (Kessler-6 score ≥13) based on the National Health Interview Survey (1997-2015), controlling for sociodemographic variables.
People with psychological distress had higher smoking prevalence and consumed more cigarettes/day than people without distress. The percentage of those with at least one quit attempt was higher among those with psychological distress. The increase in quit attempts over time was similar among smokers in each of the distress levels. For every 10 years, the OR of a quit attempt increased by a factor of 1.13 (95% CI=1.02, 1.24, p<0.05). Consumption declined by 3.35 (95% CI= -3.94, -2.75, p<0.01) cigarettes/day for those with serious psychological distress.
Although smoking more heavily than the general population, smokers with psychological distress, like the general population, are softening over time. To improve health outcomes and increase health equity, tobacco control policies should continue moving all subgroups of smokers down these softening curves, while simultaneously incorporating appropriately tailored quitting help into mental health settings.
有人认为,随着吸烟率的下降,剩下的吸烟者代表了一群“顽固”的人,他们不愿意或无法戒烟,这个过程被称为“硬化”。然而,正如最近所显示的,普通吸烟人群正在软化而不是硬化(即,随着流行率的下降,更多的戒烟尝试和继续吸烟的人消费减少)。有心理困扰的人吸烟更多,因此他们可能代表顽固的吸烟者。
使用横断面时间序列分析,根据全国健康访谈调查(1997-2015 年),在严重心理困扰(Kessler-6 评分≥13)的吸烟者中,评估了 19 年来戒烟尝试和香烟消费的变化,控制了社会人口统计学变量。
有心理困扰的人吸烟率更高,每天吸烟量也多于没有困扰的人。有心理困扰的人至少有一次戒烟尝试的比例较高。随着时间的推移,每个心理困扰水平的吸烟者戒烟尝试的增加情况相似。每增加 10 年,戒烟尝试的几率增加 1.13 倍(95%置信区间=1.02,1.24,p<0.05)。对于有严重心理困扰的人,每天的吸烟量减少了 3.35 支(95%置信区间=-3.94,-2.75,p<0.01)。
尽管吸烟量比一般人群多,但有心理困扰的吸烟者,与一般人群一样,随着时间的推移正在软化。为了改善健康结果和增加健康公平性,烟草控制政策应继续推动所有吸烟人群沿着这些软化曲线下降,同时在心理健康环境中纳入适当定制的戒烟帮助。