Department of Cardiology, Medical University of Vienna, Vienna, Austria.
Department of Cardiology, Medical University of Vienna, Vienna, Austria.
JACC Heart Fail. 2017 Nov;5(11):795-801. doi: 10.1016/j.jchf.2017.08.005. Epub 2017 Oct 11.
This study sought to compare the prognostic power of left ventricular end-diastolic pressure (LVEDP) and pulmonary arterial wedge pressure (PAWP) in heart failure with preserved ejection fraction (HFpEF).
It is broadly accepted that direct measurement of LVEDP in HFpEF more robustly reflects left ventricular hemodynamics than PAWP.
A total of 173 consecutive HFpEF patients were prospectively enrolled. Of these, 152 patients fulfilled registry inclusion criteria. Study participants underwent clinical evaluation, lung function tests, echocardiography, cardiac magnetic resonance, coronary angiography, and invasive hemodynamic assessments with PAWP and LVEDP measurements in 1 procedure. The study endpoint was defined as hospitalization for heart failure or cardiac death.
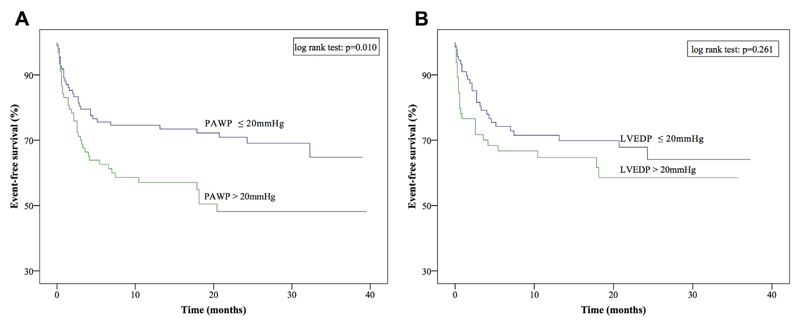
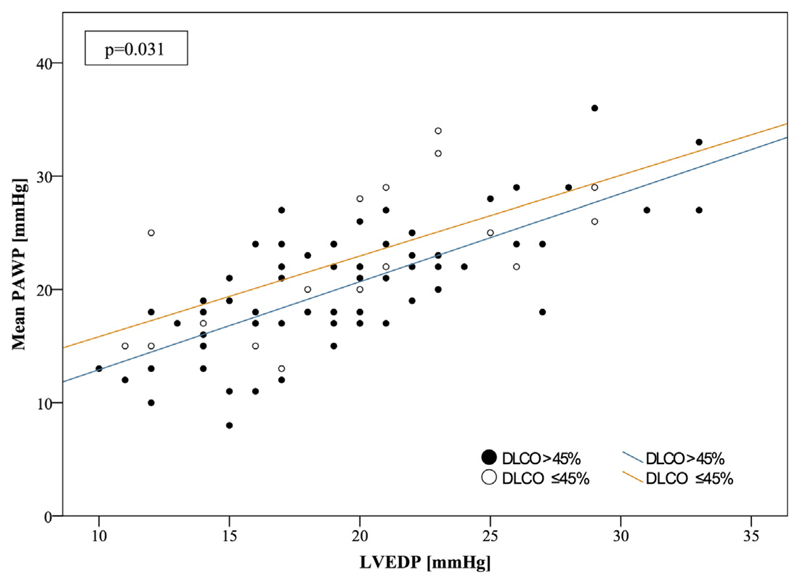
A modest pressure difference (2.0 ± 4.4 mm Hg) was observed between PAWP (21.5 ± 5.6 mm Hg) and LVEDP (19.5 ± 5.2 mm Hg) at baseline. After a mean follow-up of 23.5 ± 21.3 months, PAWP was predictive of outcome (p = 0.010), whereas LVEDP was not (p = 0.261) by Kaplan-Meier curves. By multivariate regression analysis, diffusion capacity of carbon monoxide (DLCO) was the only parameter that was independently related to the pressure difference between PAWP and LVEDP. When patients were stratified according to DLCO between ≤45% and >45%, those in the low DLCO group were found to have a more pronounced pressure drop between PAWP and LVEDP (3.1 ± 4.8 mm Hg vs. 0.8 ± 3.8 mm Hg, respectively; p = 0.031) and to be in more advanced disease stages.
Our data indicate that PAWP but not LVEDP is associated with outcome in HFpEF. A more pronounced difference between PAWP and LVEDP and more advanced disease is found in patients with low DLCO.
本研究旨在比较舒张末期左心室压(LVEDP)和肺动脉楔压(PAWP)在射血分数保留型心力衰竭(HFpEF)中的预后价值。
人们普遍认为,HFpEF 中直接测量 LVEDP 比 PAWP 更能反映左心室血流动力学。
共前瞻性纳入 173 例连续 HFpEF 患者。其中 152 例患者符合登记标准。研究参与者接受了临床评估、肺功能检查、超声心动图、心脏磁共振、冠状动脉造影和有创血流动力学评估,在 1 次操作中测量 PAWP 和 LVEDP。研究终点定义为因心力衰竭或心脏死亡而住院。
在基线时,PAWP(21.5 ± 5.6 mm Hg)和 LVEDP(19.5 ± 5.2 mm Hg)之间观察到适度的压力差(2.0 ± 4.4 mm Hg)。在平均 23.5 ± 21.3 个月的随访后,PAWP 预测结局(p = 0.010),而 LVEDP 则无此作用(p = 0.261)(Kaplan-Meier 曲线)。通过多变量回归分析,一氧化碳弥散量(DLCO)是唯一与 PAWP 和 LVEDP 之间压力差相关的参数。当根据 DLCO 将患者分为≤45%和>45%两组时,发现低 DLCO 组 PAWP 和 LVEDP 之间的压力下降更为显著(分别为 3.1 ± 4.8 mm Hg 和 0.8 ± 3.8 mm Hg;p = 0.031),且疾病处于更晚期。
我们的数据表明,PAWP 而不是 LVEDP 与 HFpEF 的结局相关。在 DLCO 较低的患者中,PAWP 和 LVEDP 之间的差异更大,疾病也更严重。