Komici Klara, Vitale Dino F, Leosco Dario, Mancini Angela, Corbi Graziamaria, Bencivenga Leonardo, Mezzani Alessandro, Trimarco Bruno, Morisco Carmine, Ferrara Nicola, Rengo Giuseppe
Division of Geriatrics, Department of Translational Medical Sciences, University of Naples Federico II, Naples, Italy.
Cardiac Rehabilitation Division, Salvatore Maugeri Foundation, IRCCS, Scientific Institute of Telese Terme (BN), Telese Terme, Italy.
Clin Interv Aging. 2017 Sep 19;12:1495-1501. doi: 10.2147/CIA.S135676. eCollection 2017.
To assess pressure injury (PI) incidence among patients hospitalized for acute myocardial infarction (AMI) in an intensive coronary care unit (ICCU) and to detect the impact of specific risk factors on the development of PI in this clinical setting.
Prospective cohort study in ICCU setting. Patients admitted for AMI: patients mean age 67.5±11.5 years (n=165). Norton Scale, Mini Nutritional Assessment (MNA), demographic, clinical and biochemical data collected at the time of ICCU admission have been tested in a logistic model to assess the odds ratios (ORs) of PI risk development. The jackknifed area under the receiver operating characteristic curve (AUC) and the decision curve analysis have been employed to assess the additive predictive value of a factor.
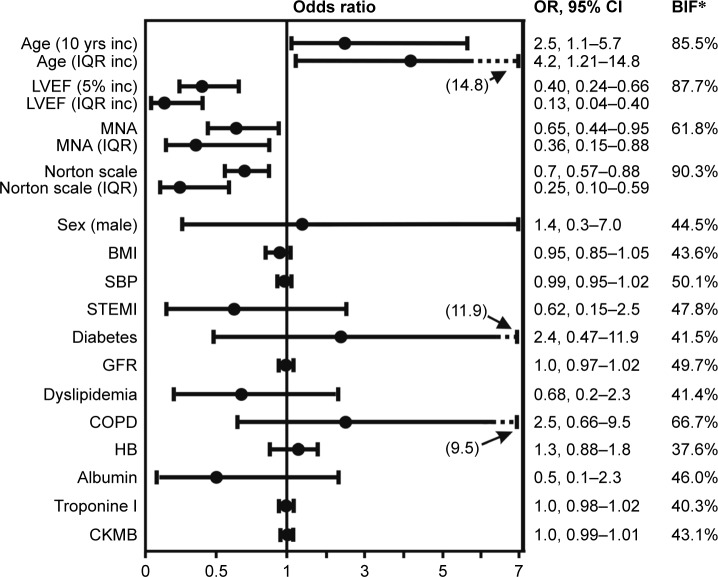
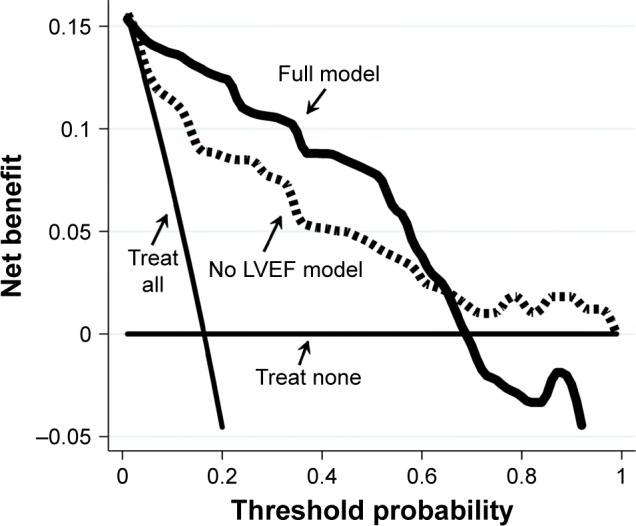
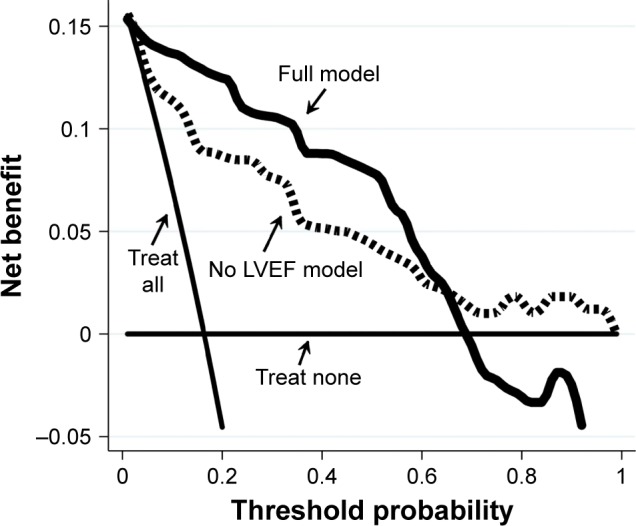
Twenty-seven (16.3%) patients developed PIs. An increased PI risk was associated with advanced age (OR =2.5 every 10-year increase; 95% CI =1.1-5.7), while probability of PI development was reduced in patients with higher left ventricular ejection fraction (LVEF) (OR =0.4 every 5% increase; 95% CI =0.24-0.66), MNA score (OR =0.65 every unit change; 95% CI =0.44-0.95) and Norton Scale score (OR =0.7 every unit change; 95% CI =0.57-0.88). The AUC and the decision curve analysis showed that LVEF inclusion improved the discrimination power and the clinical net benefit of the final model.
Age, LVEF, Norton Scale and MNA scores have a strong and independent clinical value as predictors of in-hospital PI development in patients with AMI. This finding has the potential to improve the clinical management of patients admitted in ICCU.
评估在重症冠心病监护病房(ICCU)因急性心肌梗死(AMI)住院患者的压疮(PI)发生率,并检测特定风险因素对该临床环境下压疮发生发展的影响。
在ICCU环境下进行前瞻性队列研究。因AMI入院的患者:平均年龄67.5±11.5岁(n = 165)。在逻辑模型中对ICCU入院时收集的诺顿量表、微型营养评定法(MNA)、人口统计学、临床和生化数据进行了测试,以评估压疮风险发生的比值比(OR)。采用受试者操作特征曲线(AUC)下的刀切法面积和决策曲线分析来评估一个因素的附加预测价值。
27例(16.3%)患者发生了压疮。压疮风险增加与高龄相关(每增加10岁,OR = 2.5;95%置信区间[CI] = 1.1 - 5.7),而左心室射血分数(LVEF)较高的患者发生压疮的概率降低(每增加5%,OR = 0.4;95% CI = 0.24 - 0.66),MNA评分(每单位变化,OR = 0.65;95% CI = 0.44 - 0.95)和诺顿量表评分(每单位变化,OR = 0.7;95% CI = 0.57 - 0.88)。AUC和决策曲线分析表明,纳入LVEF可提高最终模型的判别能力和临床净效益。
年龄、LVEF、诺顿量表和MNA评分作为AMI患者院内压疮发生发展的预测指标具有强大且独立的临床价值。这一发现有可能改善ICCU收治患者的临床管理。