Beltran Ralph, Veneziano Giorgio, Bhalla Tarun, Kenney Brian, Tumin Dmitry, Bissonnette Bruno, Tobias Joseph D
Department of Anesthesiology and Pain Medicine, Nationwide Children's Hospital, Columbus, Ohio, USA.
Department of Anesthesiology, The Ohio State University, Columbus, Ohio, USA.
Saudi J Anaesth. 2017 Oct-Dec;11(4):427-431. doi: 10.4103/sja.SJA_339_17.
Although the Nuss procedure provides excellent cosmetic results for the correction of pectus excavatum, the provision of analgesia following such procedures can be challenging.
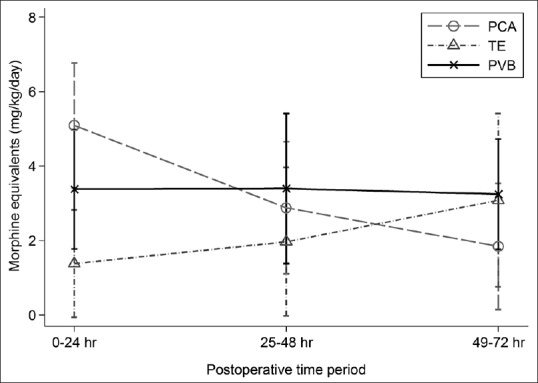
The current study retrospectively reviews our experience over a 2.5 year period with thoracic epidural analgesia (TE), paravertebral blockade (PVB), and intravenous opioids delivered via patient-controlled analgesia (PCA) to provide postoperative analgesia.
The study cohort included 30 patients (mean age = 15.6 ± 1.5 years), 15 of whom were treated with PCA, 8 with TE, and 7 with PVB. There were no significant differences in pain scores between the 3 groups at any time point during the first 3 postoperative days. Compared to PCA, the PVB group had lower opioid consumption over the first 24 hours of hospitalization by 1.7 mg/kg morphine equivalents (95% CI of difference: 0.1, 3.3; p=0.035); but had higher opioid consumption by 2.0 mg/kg morphine equivalents than the TE group (95% CI of difference: 0.3, 3.7; p=0.024). There were no differences in opioid consumption between PVB and PCA or between PVB and TE at 48 or 72 hours. The number of intraoperative hypotension episodes was significantly lower in the PCA group when compared to the PVB group (p=0.001), with no difference between the PVB and TE groups.
The use of regional anesthesia should be considered a viable option for the relief of postoperative pain in pediatric patients following the Nuss procedure albeit with a higher incidence of intraoperative hemodynamic effects. A randomized, prospective, study powered to compare all 3 techniques against one another would be necessary to confirm the significance of these findings.
尽管努斯手术在漏斗胸矫正方面能带来出色的美容效果,但术后镇痛颇具挑战性。
本研究回顾了我们在2.5年期间采用胸段硬膜外镇痛(TE)、椎旁阻滞(PVB)以及通过患者自控镇痛(PCA)给予静脉阿片类药物进行术后镇痛的经验。
研究队列包括30例患者(平均年龄 = 15.6 ± 1.5岁),其中15例接受PCA治疗,8例接受TE治疗,7例接受PVB治疗。术后前3天的任何时间点,3组之间的疼痛评分均无显著差异。与PCA相比,PVB组在住院的前24小时内阿片类药物消耗量低1.7毫克/千克吗啡当量(差异的95%置信区间:0.1,3.3;p = 0.035);但比TE组的阿片类药物消耗量高2.0毫克/千克吗啡当量(差异的95%置信区间:0.3,3.7;p = 0.024)。在48或72小时时,PVB与PCA之间以及PVB与TE之间的阿片类药物消耗量无差异。与PVB组相比,PCA组术中低血压发作次数显著更低(p = 0.001),PVB组与TE组之间无差异。
对于接受努斯手术的儿科患者,尽管术中血流动力学影响发生率较高,但区域麻醉的使用应被视为缓解术后疼痛的可行选择。有必要进行一项随机、前瞻性研究,以比较所有这3种技术,从而证实这些发现的重要性。