Akuzawa Nobuhiro, Kurabayashi Makoto, Suzuki Tsukasa, Yoshinari Daisuke, Kobayashi Mitsunobu, Tanahashi Yoshifumi, Makita Fujio, Saito Ryusei
Departments of General Medicine, National Hospital Organization Shibukawa Medical Center, 383 Shiroi, Shibukawa, Gunma, 377-0280, Japan.
Surgery, National Hospital Organization Shibukawa Medical Center, 383 Shiroi, Shibukawa, Gunma, 377-0280, Japan.
Diagn Pathol. 2017 Oct 16;12(1):74. doi: 10.1186/s13000-017-0664-x.
Spontaneous isolated dissection of the superior mesenteric artery (SMA) can lead to bowel ischemia, aneurysm rupture, or even death. Studies have suggested that mechanical or hemodynamic stress on the vascular wall of the SMA may be a contributor, but its pathogenesis is unclear.
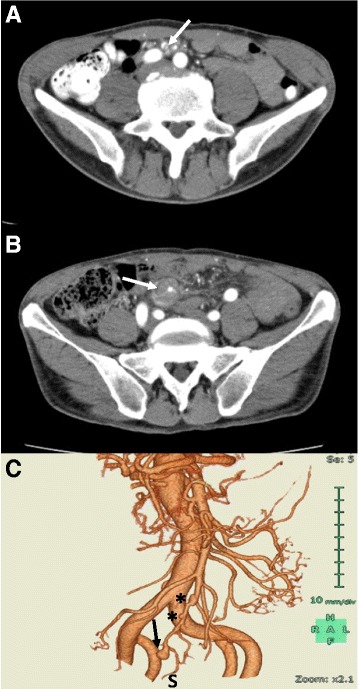
A 57-year-old Japanese man with a history of untreated hypertension and hyperuricemia was admitted to our hospital with the sudden onset of severe epigastric pain. Laboratory findings showed elevated white blood cell count and C-reactive protein, and contrast-enhanced computed tomography (CT) of the abdomen demonstrated arterial dissection with luminal stenosis and aneurysm formation at the distal portion of the SMA after the branching of the jejunal artery, and intravenous nicardipine was administered. The patient's epigastric pain resolved spontaneously but recurred on day 6 of his hospital stay. Contrast-enhanced abdominal CT revealed an enlarged aneurysm with wall thinning. Because of the risk of aneurysm rupture, the decision was made to perform aneurysmectomy and bowel resection on day 6. Histologic examinations revealed two separate dissecting lesions: one latent and the other resulting in aneurysm formation. Both lesions showed characteristics of segmental arterial mediolysis (SAM) with lack of arterial media, absence of internal and external elastic laminae and intimal proliferation.
Histologic findings in the present case suggest that mechanical or hemodynamic stress on the vascular wall and SAM-related vascular vulnerability may concomitantly contribute to the onset of isolated SMA dissection.
肠系膜上动脉(SMA)自发性孤立性夹层可导致肠缺血、动脉瘤破裂,甚至死亡。研究表明,SMA血管壁上的机械或血流动力学应激可能是一个促成因素,但其发病机制尚不清楚。
一名57岁的日本男性,有未经治疗的高血压和高尿酸血症病史,因突发严重上腹痛入院。实验室检查结果显示白细胞计数和C反应蛋白升高,腹部增强计算机断层扫描(CT)显示在空肠动脉分支后,SMA远端出现动脉夹层伴管腔狭窄和动脉瘤形成,遂给予静脉注射尼卡地平。患者的上腹痛自行缓解,但在住院第6天复发。腹部增强CT显示动脉瘤增大,壁变薄。由于存在动脉瘤破裂风险,于住院第6天决定行动脉瘤切除术和肠切除术。组织学检查发现两个独立的夹层病变:一个为潜伏性病变,另一个导致动脉瘤形成。两个病变均显示节段性动脉中层溶解(SAM)的特征,即缺乏动脉中层、内外弹性膜缺失和内膜增生。
本病例的组织学发现表明,血管壁上的机械或血流动力学应激以及与SAM相关的血管易损性可能共同促成孤立性SMA夹层的发生。