Department of Cardiology, The First Affiliated Hospital of Dalian Medical University, 222 Zhongshan Road, Dalian, 116011, People's Republic of China.
Present address: Department of Cardiology, The Fifth People's Hospital of Dalian City, Dalian, People's Republic of China.
Stem Cell Res Ther. 2017 Oct 16;8(1):231. doi: 10.1186/s13287-017-0680-5.
Several cell-based therapies for adjunctive treatment of acute myocardial infarction have been investigated in multiple clinical trials, but the timing of transplantation remains controversial. We conducted a meta-analysis of randomized controlled trials to investigate the effects of timing on bone marrow-derived cell (BMC) therapy in acute myocardial infarction (AMI).
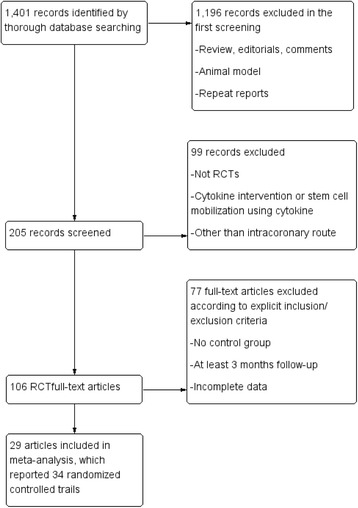
A systematic literature search of PubMed, MEDLINE, and Cochrane Evidence-Based Medicine databases from January 2000 to June 2017 was performed on randomized controlled trials with at least a 3-month follow-up for patients with AMI undergoing emergency percutaneous coronary intervention (PCI) and receiving intracoronary BMC transfer thereafter. The defined end points were left ventricular (LV) ejection fraction, LV end-diastolic and end-systolic index. The data were analyzed to evaluate the effects of timing on BMC therapy.
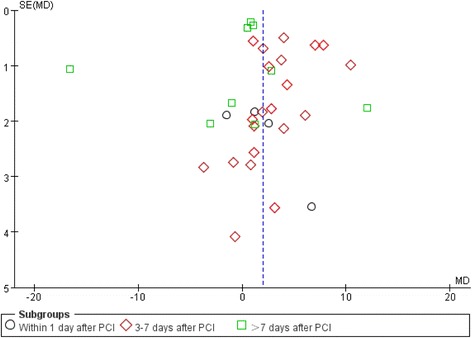
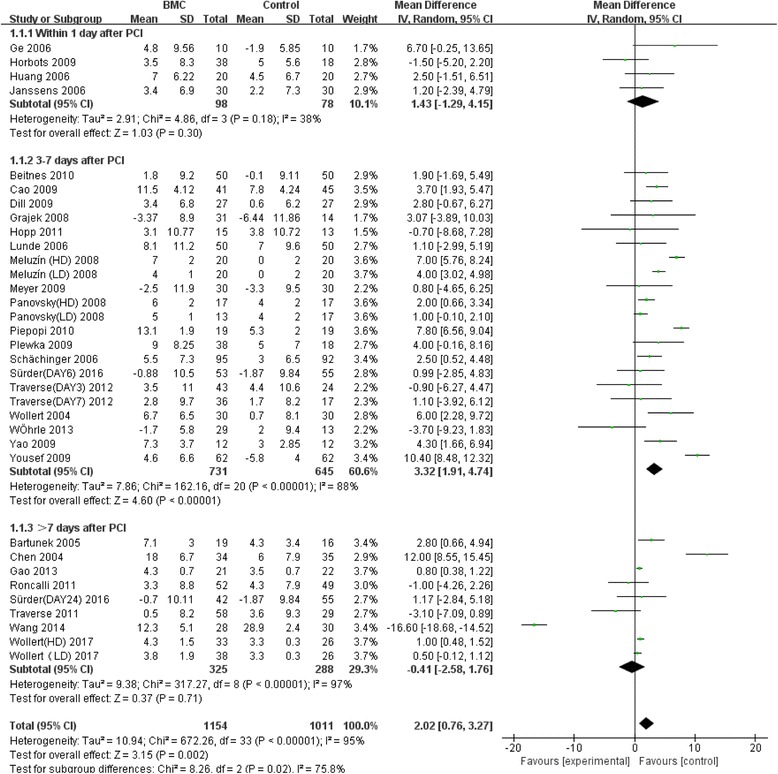
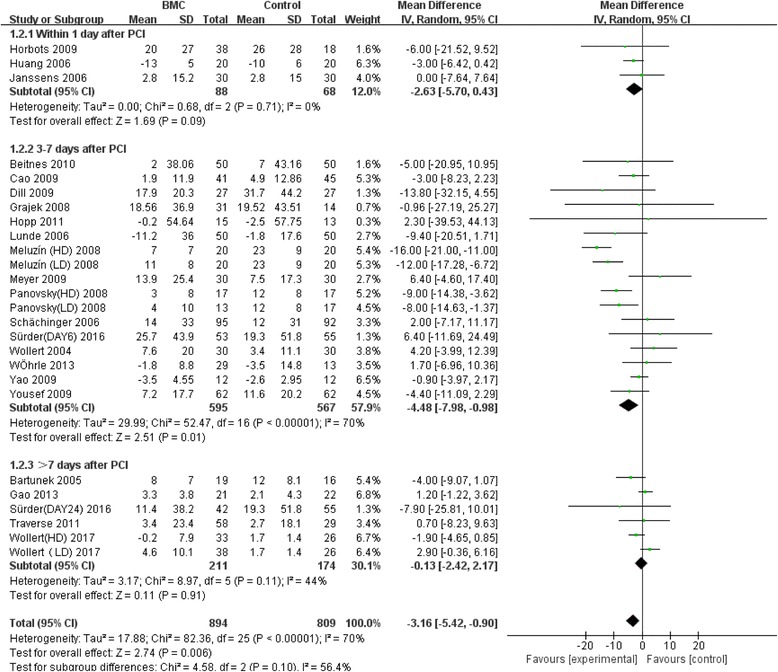
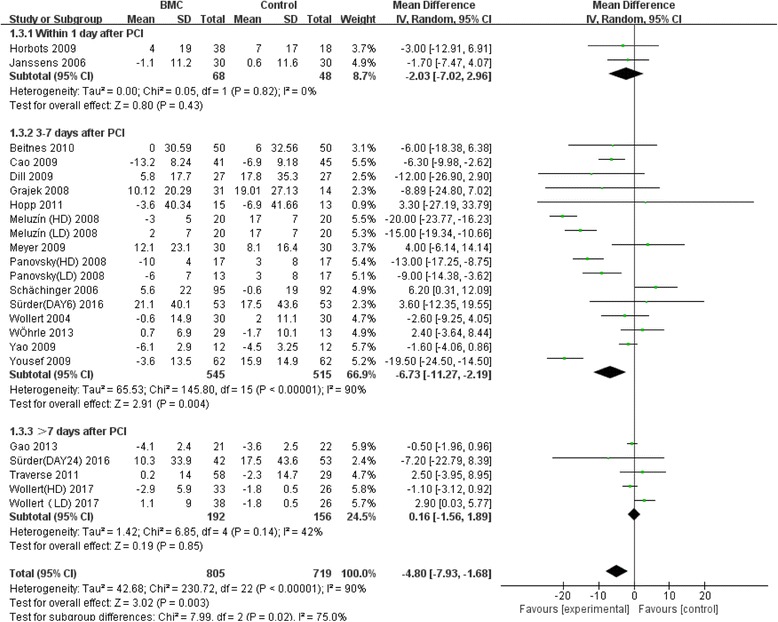
Thirty-four RCTs comprising a total of 2,307 patients were included; the results show that, compared to the control group, AMI patients who received BMC transplantation showed significantly improved cardiac function. BMC transplantation 3-7 days after PCI (+3.32%; 95% CI, 1.91 to 4.74; P < 0.00001) resulted in a significant increase of left ventricular ejection fraction (LVEF). As for the inhibitory effect on ventricular remodeling, BMC transplantation 3-7 days after PCI reduced LV end-diastolic indexes (-4.48; 95% CI, -7.98 to -0.98; P = 0.01) and LV end-systolic indexes (-6.73; 95% CI, -11.27 to -2.19; P = 0.004). However, in the groups who received BMC transplantation either within 24 hours or later than 7 days there was no significant effect on treatment outcome. In subgroup analysis, the group with LVEF ≤ 50% underwent a significant decrease in LV end-diastolic index after BMC transplantation (WMD = -3.29, 95% CI, -4.49 to -2.09; P < 0.00001); the decrease was even more remarkable in the LV end-systolic index after BMC transplantation in the group with LVEF ≤ 50% (WMD = -5.25, 95% CI, -9.30 to -1.20; P = 0.01), as well as in patients who received a dose of 10^7-10^8 cells (WMD = -12.99, 95% CI, -19.07 to -6.91; P < 0.0001). In the group with a follow-up of more than 12 months, this beneficial effect was significant and increased to a more pronounced effect of +3.58% (95% CI, 1.55 to 5.61; P = 0.0006) when compared with control.
In this meta-analysis, BMC transfer at 3 to 7 days post-AMI was superior to transfer within 24 hours or more than 7 days after AMI in improving LVEF and decreasing LV end-systolic dimensions or LV end-diastolic dimensions. It is more effective in patients with lower baseline LVEF (≤50%) and the effect can last more than 12 months.
多项临床试验研究了几种细胞疗法作为急性心肌梗死的辅助治疗方法,但移植时机仍存在争议。我们对随机对照试验进行了荟萃分析,以调查骨髓源性细胞(BMC)治疗急性心肌梗死(AMI)时时机的影响。
对 2000 年 1 月至 2017 年 6 月期间的PubMed、MEDLINE 和 Cochrane 循证医学数据库进行了系统的文献检索,纳入了至少随访 3 个月的接受紧急经皮冠状动脉介入治疗(PCI)并随后接受冠状动脉内 BMC 转移的 AMI 患者的随机对照试验。定义的终点是左心室(LV)射血分数、LV 舒张末期和收缩末期指数。分析数据以评估时机对 BMC 治疗的影响。
共纳入 34 项 RCT,总计 2307 例患者。结果表明,与对照组相比,接受 BMC 移植的 AMI 患者心脏功能明显改善。PCI 后 3-7 天进行 BMC 移植(增加 3.32%;95%CI,1.91 至 4.74;P < 0.00001)可显著提高左心室射血分数(LVEF)。至于对心室重构的抑制作用,PCI 后 3-7 天进行 BMC 移植可降低 LV 舒张末期指数(-4.48;95%CI,-7.98 至 -0.98;P = 0.01)和 LV 收缩末期指数(-6.73;95%CI,-11.27 至 -2.19;P = 0.004)。然而,在接受 BMC 移植的 24 小时内或 7 天后的组中,治疗结果没有显著影响。亚组分析显示,LVEF≤50%的组在 BMC 移植后 LV 舒张末期指数显著下降(WMD = -3.29,95%CI,-4.49 至 -2.09;P < 0.00001);LVEF≤50%的组在 BMC 移植后 LV 收缩末期指数的下降更为明显(WMD = -5.25,95%CI,-9.30 至 -1.20;P = 0.01),以及接受 10^7-10^8 个细胞剂量的患者(WMD = -12.99,95%CI,-19.07 至 -6.91;P < 0.0001)。在随访时间超过 12 个月的组中,与对照组相比,这种有益的效果更为显著,增加至更明显的+3.58%(95%CI,1.55 至 5.61;P = 0.0006)。
在这项荟萃分析中,AMI 后 3 至 7 天进行 BMC 转移比在 AMI 后 24 小时内或超过 7 天进行转移在提高 LVEF 和降低 LV 收缩末期或舒张末期尺寸方面更具优势。对于基线 LVEF 较低(≤50%)的患者更有效,且效果可持续超过 12 个月。