Barnes Edward L, Kochar Bharati, Long Millie D, Martin Christopher F, Crockett Seth D, Korzenik Joshua R, Kappelman Michael D
Division of Gastroenterology and Hepatology, University of North Carolina at Chapel Hill, Chapel Hill, NC.
Division of Gastroenterology and Hepatology, University of North Carolina at Chapel Hill, Chapel Hill, NC.
J Pediatr. 2017 Dec;191:184-189.e1. doi: 10.1016/j.jpeds.2017.08.042. Epub 2017 Oct 14.
To evaluate the burden and predictors of hospital readmissions among pediatric patients with inflammatory bowel disease using the Nationwide Readmissions Database.
We performed a retrospective cohort study using 2013 Nationwide Readmissions Database. International Classification of Diseases, Ninth Revision, Clinical Modification codes were used to identify patients <18 years with diagnoses of ulcerative colitis (UC) or Crohn's disease (CD). Demographic factors and details of hospitalizations were evaluated using survey procedures in SAS v 9.4 (SAS Institute, Cary, North Carolina). Multivariable logistic regression was used to estimate ORs and 95% CIs of readmission.
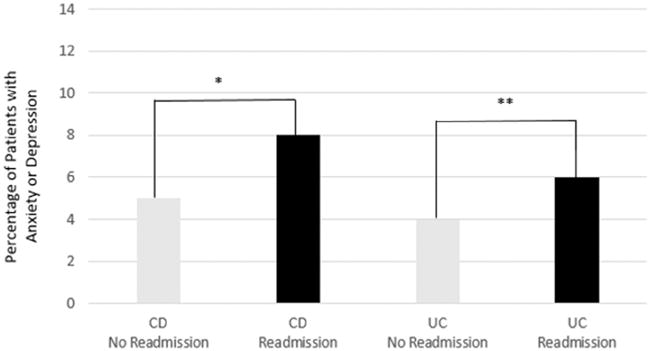
Among 2733 hospitalizations (63% CD, 37% UC), 611 (22%) patients were readmitted within 90 days of the index hospitalization. Readmission resulted in weighted estimates of 11 440 excess days of hospitalization and total charges of over $107 million. For CD, male sex (aOR 1.36, 95% CI 1.03-1.81) and co-existing anxiety or depression (aOR 1.89, 95% CI 1.06-3.40) were associated with increased readmissions, while patients who underwent surgery had decreased readmissions (aOR 0.40, 95% CI 0.24-0.65). In patients with UC, an index admission of >7 days was associated with increased readmissions (aOR 1.69, 95% CI 1.09-2.62).
Readmission occurs frequently in children with inflammatory bowel disease and is associated with significant cost and resource burdens. Among patients with CD, psychiatric comorbidities such as anxiety and depression are apparent drivers of readmission.
使用全国再入院数据库评估炎症性肠病儿科患者再次入院的负担及预测因素。
我们利用2013年全国再入院数据库进行了一项回顾性队列研究。采用国际疾病分类第九版临床修订本编码来识别年龄小于18岁、诊断为溃疡性结肠炎(UC)或克罗恩病(CD)的患者。使用SAS v 9.4(SAS研究所,北卡罗来纳州卡里)中的调查程序评估人口统计学因素和住院细节。采用多变量逻辑回归来估计再次入院的比值比(OR)和95%可信区间(CI)。
在2733例住院病例中(63%为CD,37%为UC),611例(22%)患者在首次住院后的90天内再次入院。再次入院导致加权估计额外住院天数达11440天,总费用超过1.07亿美元。对于CD,男性(调整后OR为1.36,95%CI为1.03 - 1.81)以及并存焦虑或抑郁(调整后OR为1.89,95%CI为1.06 - 3.40)与再次入院增加相关,而接受手术的患者再次入院率降低(调整后OR为0.40,95%CI为0.24 - 0.65)。在UC患者中,首次住院时间>7天与再次入院增加相关(调整后OR为1.69,95%CI为1.09 - 2.62)。
炎症性肠病患儿频繁出现再次入院情况,且与巨大的成本和资源负担相关。在CD患者中,焦虑和抑郁等精神共病是再次入院的明显驱动因素。