Hospital Pharmacy Research Unit, Department of Regional Health Research-IRS, Hospital Sønderjylland, University Hospital of Southern Denmark, Aabenraa, Denmark.
National Center of Excellence for Molecular Prediction of Inflammatory Bowel Disease- PREDICT, Department of Clinical Medicine, Faculty of Medicine, Aalborg University, Copenhagen, Denmark.
Syst Rev. 2024 Jun 24;13(1):164. doi: 10.1186/s13643-024-02584-3.
Inflammatory bowel diseases (IBDs) are associated with high healthcare utilization. This systematic review aimed to summarize what is known about the impact of sex, income, and education on the likelihood of bowel surgery, hospitalization, and use of corticosteroids and biologics among patients with IBD.
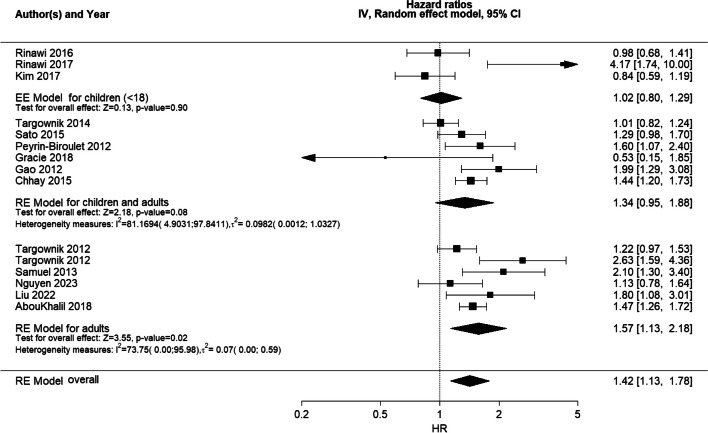
We used EMBASE, MEDLINE, CINAHL, and Web of Science to perform a systematic literature search. Pooled hazard ratios (HRs) and odds ratios (ORs) with 95% confidence intervals (CIs) were calculated using random effects meta-analysis for the impact of sex on the likelihood of surgery and hospitalization. In addition, we performed subgroup analyses of the effect of IBD type (Crohn's disease or ulcerative colitis) and age. Finally, meta-regression was undertaken for the year of publication.
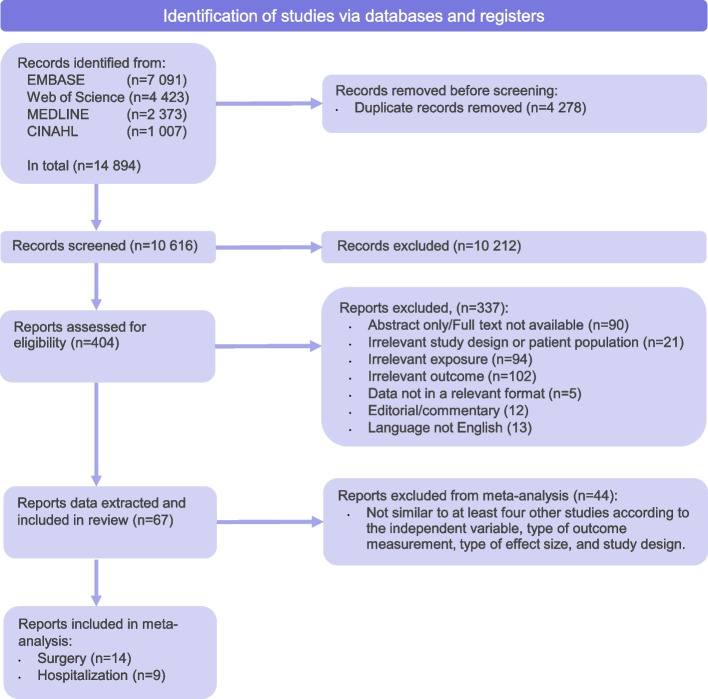
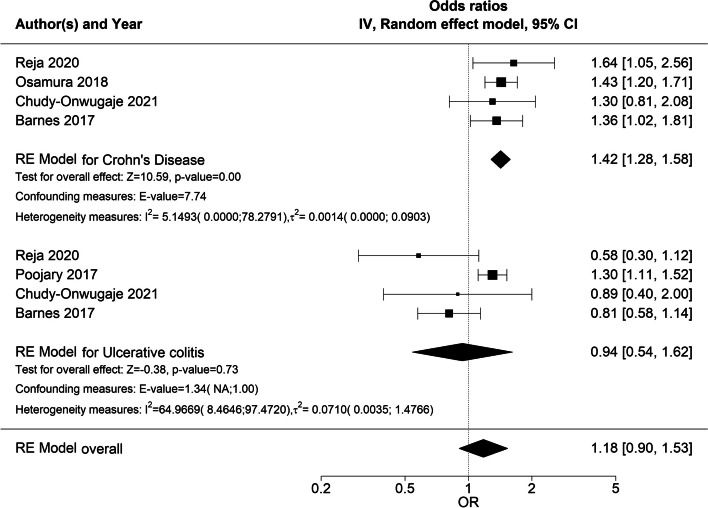
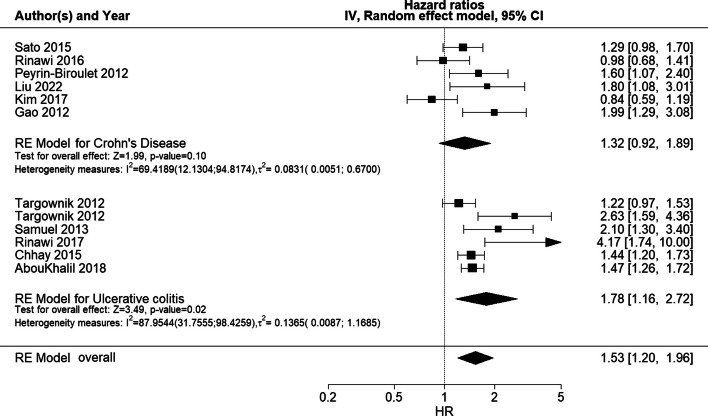
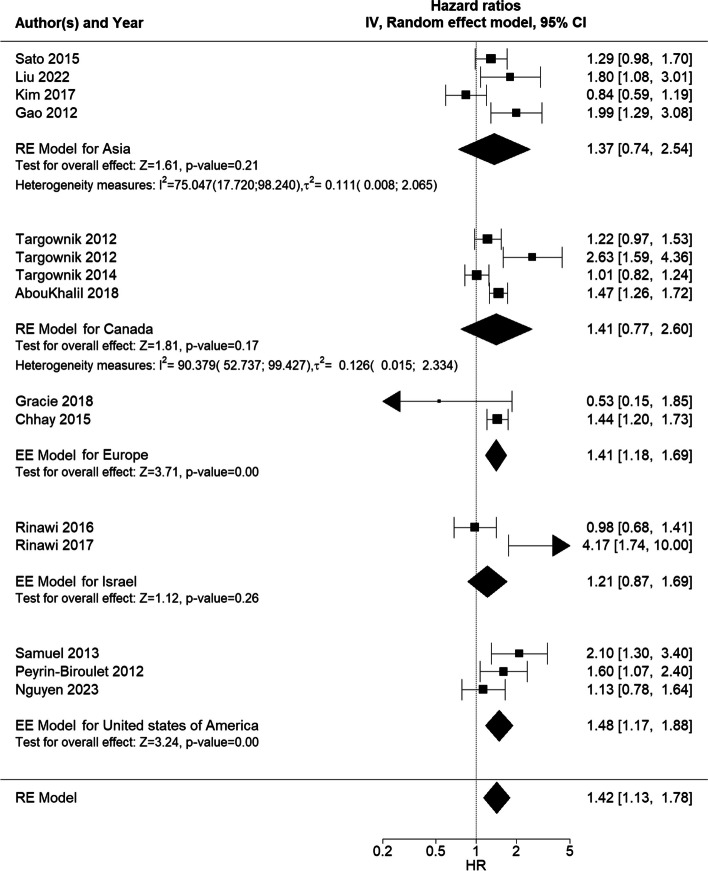
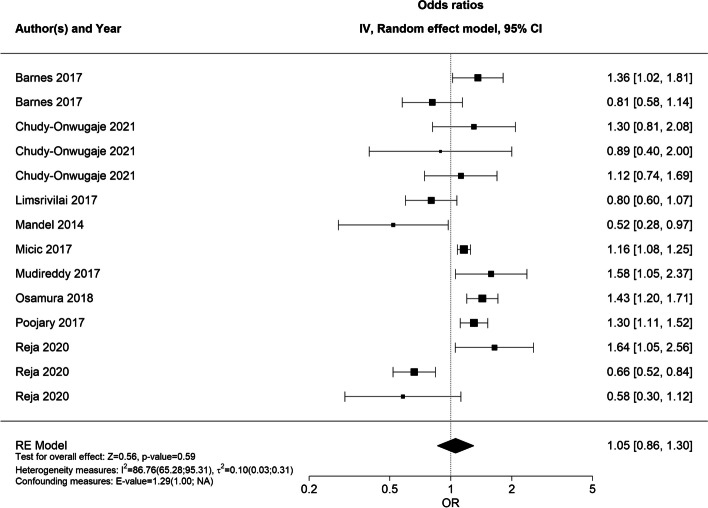
In total, 67 studies were included, of which 23 studies were eligible for meta-analysis. In the main meta-analysis, male sex was associated with an increased likelihood of bowel surgery (HR 1.42 (95% CI 1.13;1.78), which was consistent with the subgroup analysis for UC only (HR 1.78, 95% CI 1.16; 2.72). Sex did not impact the likelihood of hospitalization (OR 1.05 (95% CI 0.86;1.30), although the subgroup analysis revealed an increased likelihood of hospitalization in CD patients (OR 1.42, 95% CI 1.28;1.58). In 9 of 10 studies, no significant sex-based differences in the use of biologics were reported, although in 6 of 6 studies, female patients had lower adherence to biologics. In 11 of 13 studies, no significant sex-based difference in the use of corticosteroids was reported. The evidence of the impact of income and education on healthcare utilization was sparse and pointed in different directions. The substantial heterogeneity between studies was explained, in part, by differences in IBD type and age.
The results of this systematic review indicate that male patients with IBD are significantly more likely to have surgery than female patients with IBD but are not, overall, more likely to be hospitalized, whereas female patients appear to have statistically significantly lower adherence to biologics compared to male patients. Thus, clinicians should not underestimate the impact of sex on healthcare utilization. Evidence for income- and education-based differences remains sparse.
PROSPERO CRD42022315788.
炎症性肠病(IBD)与高医疗保健利用率相关。本系统评价旨在总结性别、收入和教育对 IBD 患者接受肠手术、住院、皮质类固醇和生物制剂治疗可能性的影响。
我们使用 EMBASE、MEDLINE、CINAHL 和 Web of Science 进行系统文献检索。使用随机效应荟萃分析计算性别对手术和住院可能性的影响的汇总风险比(HR)和优势比(OR)。此外,我们还对 IBD 类型(克罗恩病或溃疡性结肠炎)和年龄的影响进行了亚组分析。最后,我们对出版物年份进行了元回归分析。
共纳入 67 项研究,其中 23 项研究符合纳入标准。在主要的荟萃分析中,男性性别与肠手术可能性增加相关(HR 1.42(95%CI 1.13;1.78),这与仅溃疡性结肠炎的亚组分析结果一致(HR 1.78,95%CI 1.16;2.72)。性别并不影响住院的可能性(OR 1.05(95%CI 0.86;1.30),尽管亚组分析显示 CD 患者的住院可能性增加(OR 1.42,95%CI 1.28;1.58)。在 10 项研究中的 9 项中,报告的生物制剂使用不存在显著的性别差异,尽管在 6 项研究中,女性患者对生物制剂的依从性较低。在 13 项研究中的 11 项中,报告的皮质类固醇使用不存在显著的性别差异。关于收入和教育对医疗保健利用的影响的证据很少,而且指向不同的方向。研究之间的显著异质性部分可以通过 IBD 类型和年龄的差异来解释。
本系统评价的结果表明,与女性 IBD 患者相比,男性 IBD 患者更有可能接受手术,但总体而言,他们不太可能住院,而女性患者对生物制剂的依从性似乎明显低于男性患者。因此,临床医生不应低估性别的医疗保健利用的影响。关于收入和教育基础差异的证据仍然很少。
PROSPERO CRD42022315788。