Clinical Research Unit, Italian Institute of Telemedicine, Varese, Italy.
Division of Cardiovascular Medicine, Department of Medicine, Jichi Medical University School of Medicine, Shimotsuke, Japan.
J Hypertens. 2018 Apr;36(4):720-733. doi: 10.1097/HJH.0000000000001608.
To evaluate the impact of olmesartan alone or combined with one to three antihypertensive drugs on 24-h blood pressure variability (BPV) and on distribution of BP reduction in a pooled individual data analysis of 10 double-blind, randomized, ambulatory BP monitoring (ABPM) studies.
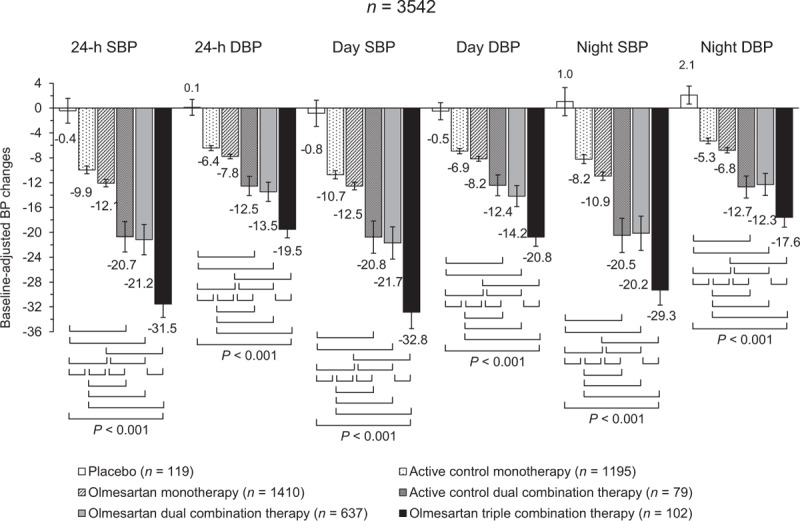
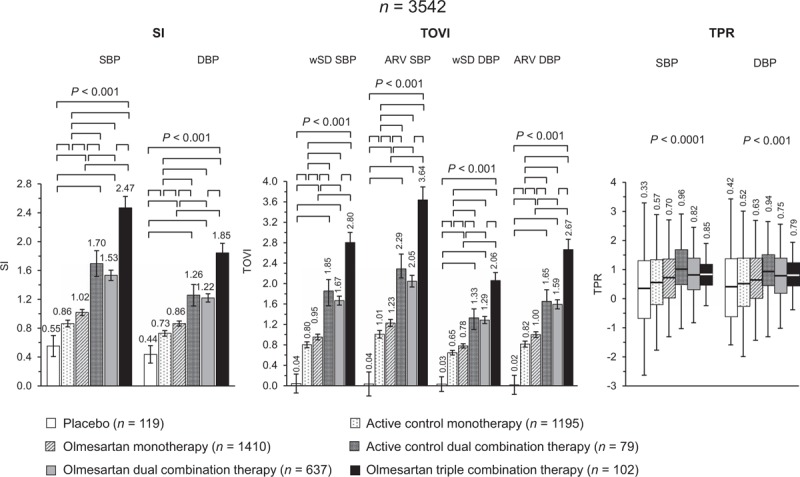
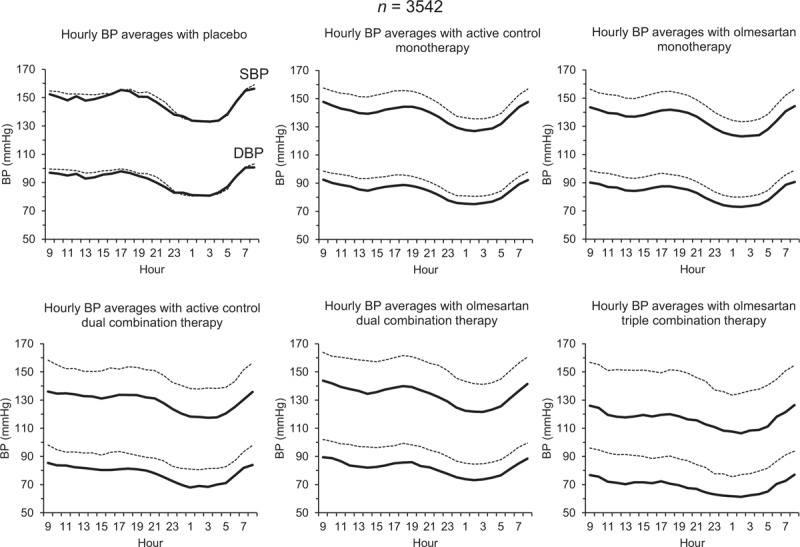
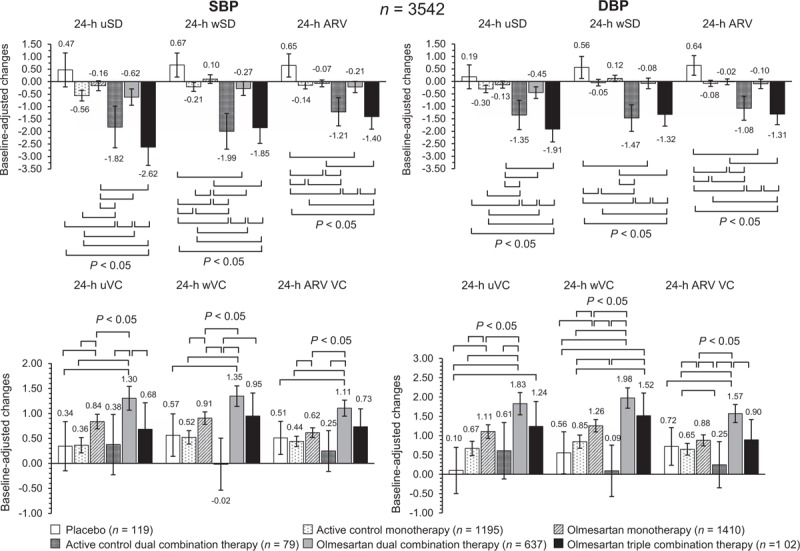
ABPMs were performed before and after 6-12 weeks of treatment with placebo (n = 119), active control monotherapy [n = 1195, angiotensin-converting enzyme inhibitors (ACEIs), angiotensin II receptor blockers (ARBs), dihydropyridine calcium channel blockers (DCCBs)] olmesartan monotherapy (n = 1410), active control dual combination [n = 79, DCCB + thiazide diuretic (TD)], olmesartan dual combination (n = 637, DCCB or TD), and triple combination therapy (n = 102, DCCB+TD). 24-h BPV was calculated as unweighted or weighted SD of the mean BP, and average real variability. BP control was assessed by smoothness index and treatment-on-variability index.
The greatest effect on 24-h systolic BPV/diastolic BPV was observed under olmesartan triple [-2.6/-1.9; -1.9/-1.3; -1.4/-1.3 mmHg] and active control dual combination [-1.8/-1.4; -1.9/-1.5; -1.2/-1.1 mmHg]. Smoothness indexes and treatment-on-variability indexes were significantly (P = 0.0001) higher under olmesartan dual (1.53/1.22, 1.67/1.29, 2.05/1.59), olmesartan triple (2.47/1.85, 2.80/2.06, 3.64/2.67), or active control dual combination (1.70/1.26, 1.85/1.33, 2.29/1.65) than under monotherapies (control: 0.86/0.73, 0.80/0.65, 1.01/0.82; olmesartan: 1.02/0.86, 0.95/0.78, 1.23/1.00). They were also greater in patients receiving high-dose olmesartan monotherapy or high-dose olmesartan dual combination than in the corresponding low-dose group.
Olmesartan plus a DCCB and/or a TD produces a larger, more sustained, and smoother BP reduction than placebo and monotherapies, a desirable feature for a more effective prevention of the cardiovascular consequences of uncontrolled hypertension.
通过对 10 项双盲、随机、动态血压监测(ABPM)研究的个体数据进行汇总分析,评估奥美沙坦单药或联合使用 1-3 种降压药对 24 小时血压变异性(BPV)的影响,并评估降压幅度的分布。
在安慰剂(n=119)、活性对照单药治疗[血管紧张素转换酶抑制剂(ACEI)、血管紧张素 II 受体阻滞剂(ARB)、二氢吡啶钙通道阻滞剂(DCCB)](n=1195)、奥美沙坦单药治疗(n=1410)、活性对照联合治疗[DCCB+噻嗪类利尿剂(TD)](n=79)、奥美沙坦联合治疗(n=637,DCCB 或 TD)和三联治疗(n=102,DCCB+TD)前后进行 ABPM,共 6-12 周。24 小时 BPV 通过未加权或加权平均 BP 的标准差和平均真实变异性来计算。通过平滑指数和治疗变异性指数评估 BP 控制情况。
奥美沙坦三联(-2.6/-1.9;-1.9/-1.3;-1.4/-1.3mmHg)和活性对照联合治疗(-1.8/-1.4;-1.9/-1.5;-1.2/-1.1mmHg)对 24 小时收缩压 BPV/舒张压 BPV 的影响最大。奥美沙坦联合治疗(1.53/1.22、1.67/1.29、2.05/1.59)、奥美沙坦三联(2.47/1.85、2.80/2.06、3.64/2.67)或活性对照联合治疗(1.70/1.26、1.85/1.33、2.29/1.65)的平滑指数和治疗变异性指数均显著高于单药治疗(对照组:0.86/0.73、0.80/0.65、1.01/0.82;奥美沙坦:1.02/0.86、0.95/0.78、1.23/1.00)。在接受高剂量奥美沙坦单药治疗或高剂量奥美沙坦联合治疗的患者中,其效果也大于相应的低剂量组。
与安慰剂和单药治疗相比,奥美沙坦加 DCCB 和/或 TD 可产生更大、更持续、更平稳的血压下降,这是更有效地预防未控制高血压的心血管后果的理想特征。