Staudacher Jonas J, Yazici Cemal, Bul Vadim, Zeidan Joseph, Khalid Ahmer, Xia Yinglin, Krett Nancy, Jung Barbara
Department of Medicine, University of Illinois at Chicago, Chicago, Illinois, USA.
Transplant Hepatology, Carolinas Medical Center, Charlotte, North Carolina, USA.
Clin Transl Gastroenterol. 2017 Oct 19;8(10):e124. doi: 10.1038/ctg.2017.48.
The basis for over-representation of colorectal cancer (CRC) in African-American (AA) populations compared with Caucasians are multifactorial and complex. Understanding the mechanisms for this racial disparity is critical for delivery of better care. Several studies have investigated sporadic CRC for differences in somatic mutations between AAs and Caucasians, but owing to small study sizes and conflicting results to date, no definitive conclusions have been reached.
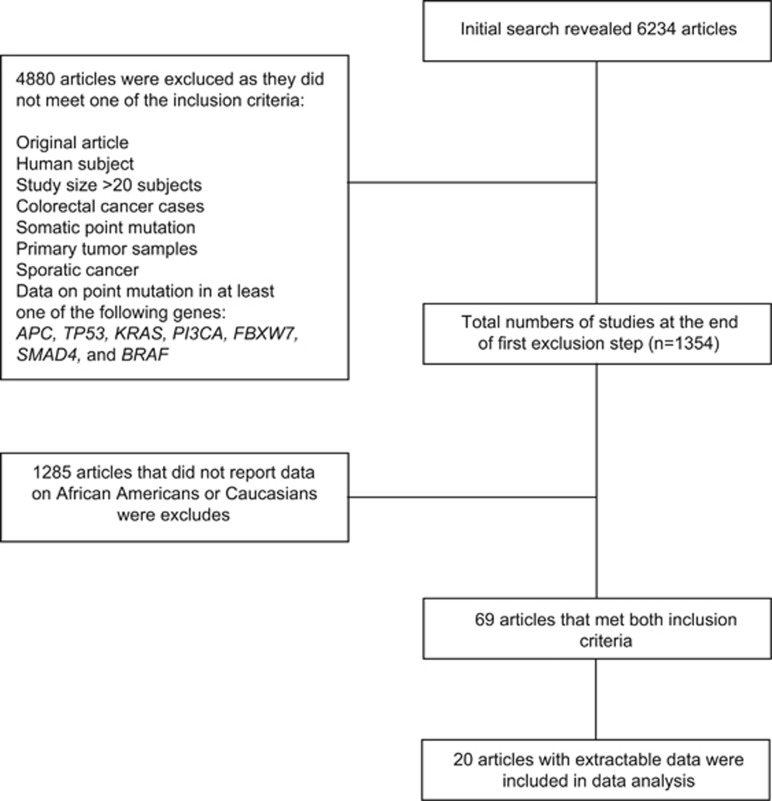
Here, we present the first systematic literature review and meta-analysis investigating the mutational differences in sporadic CRC between AAs and Caucasians focused on frequent driver mutations (APC,TP53, KRAS,PI3CA, FBXW7,SMAD4, and BRAF). Publication inclusion criteria comprised sporadic CRC, human subjects, English language, information on ethnicity (AA, Caucasian, or both), total subject number >20, and information on mutation frequencies.
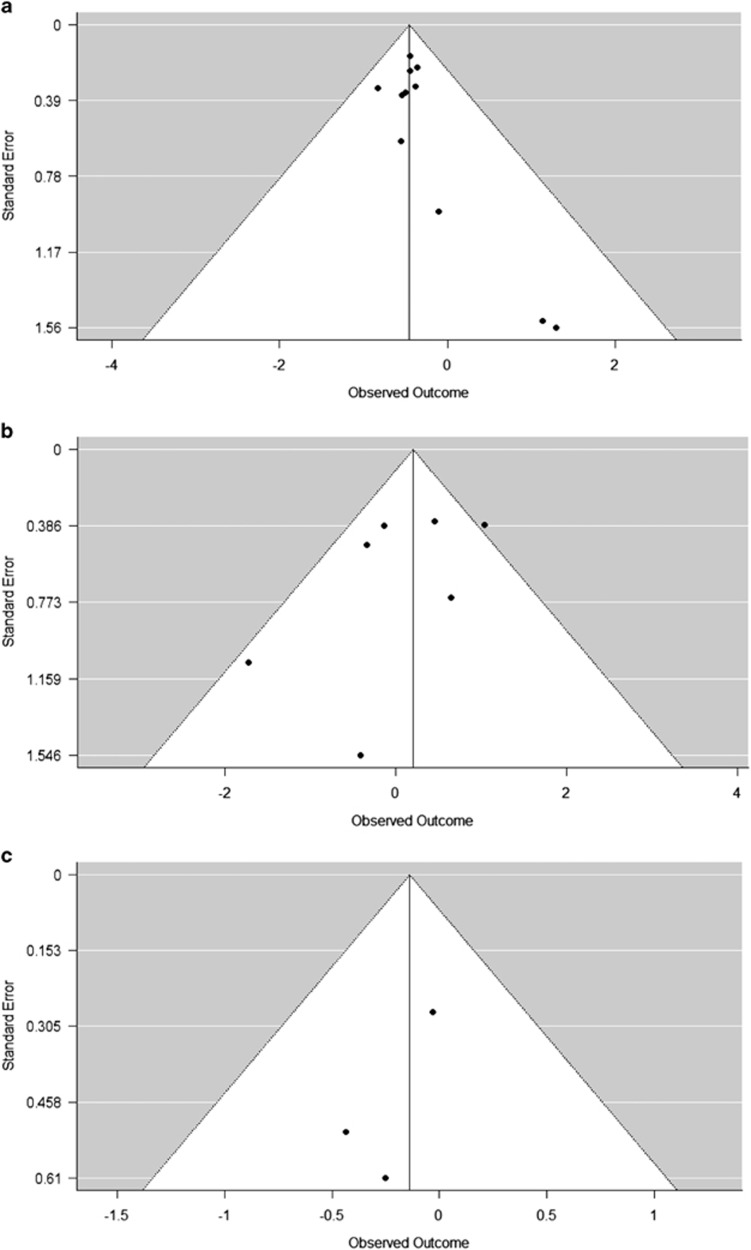
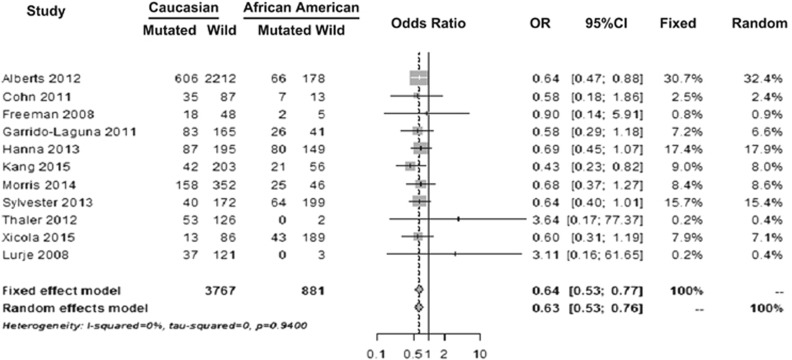
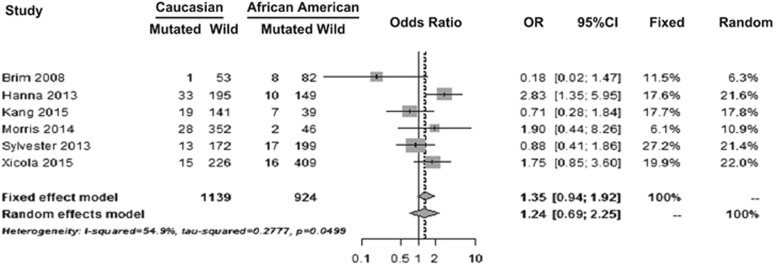
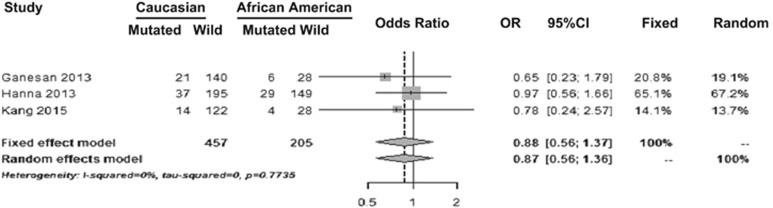
We identified 6,234 publications. Meta-analysis for APC, TP54, FBXW7, or SMAD4 was not possible owing to paucity of data. KRAS mutations were statistically less frequent in non-Hispanic Whites when compared with AAs (odds ratio, 0.640; 95% confidence interval (CI): 0.5342-0.7666; P=0.0001), while the mutational differences observed in BRAF and PI3CA did not reach statistical significance.
Here, we report the mutational patterns for KRAS, BRAF, and PI3CA in sporadic CRC of AAs and Caucasians in a systematic meta-analysis of previously published data. We identified an increase in KRAS mutations in sporadic CRC in AAs, which may contribute to worse prognosis and increased mortality of CRC in AAs. Future studies investigating health-care disparities in CRC in AAs should control for KRAS mutational frequency.
与白种人相比,非裔美国人(AA)人群中结直肠癌(CRC)发病率过高的原因是多因素且复杂的。了解这种种族差异的机制对于提供更好的医疗服务至关重要。多项研究调查了散发性CRC中AA与白种人之间体细胞突变的差异,但由于研究规模较小且结果相互矛盾,至今尚未得出明确结论。
在此,我们首次进行了系统的文献综述和荟萃分析,研究AA与白种人散发性CRC中频繁驱动突变(APC、TP53、KRAS、PI3CA、FBXW7、SMAD4和BRAF)的突变差异。纳入标准包括散发性CRC、人类受试者、英文文献、种族信息(AA、白种人或两者)、总受试者数量>20以及突变频率信息。
我们共识别出6234篇文献。由于数据匮乏,无法对APC、TP54、FBXW7或SMAD4进行荟萃分析。与AA相比,非西班牙裔白人中KRAS突变在统计学上的发生频率较低(优势比,0.640;95%置信区间(CI):0.5342 - 0.7666;P = 0.0001),而BRAF和PI3CA中观察到的突变差异未达到统计学显著性。
在此,我们通过对先前发表数据的系统荟萃分析,报告了AA和白种人散发性CRC中KRAS、BRAF和PI3CA的突变模式。我们发现AA散发性CRC中KRAS突变增加,这可能导致AA中CRC预后更差和死亡率增加。未来研究AA中CRC医疗保健差异时应控制KRAS突变频率。