Vryonidou Andromachi, Paschou Stavroula A, Dimitropoulou Fotini, Anagnostis Panagiotis, Tzavara Vasiliki, Katsivas Apostolos
Department of Endocrinology and Diabetes, Hellenic Red Cross Hospital, Athens, Greece.
Unit of Reproductive Endocrinology, First Department of Obstetrics and Gynecology, Medical School, Aristotle University of Thessaloniki, Thessaloniki, Greece.
Endocrinol Diabetes Metab Case Rep. 2017 Oct 13;2017. doi: 10.1530/EDM-17-0097. eCollection 2017.
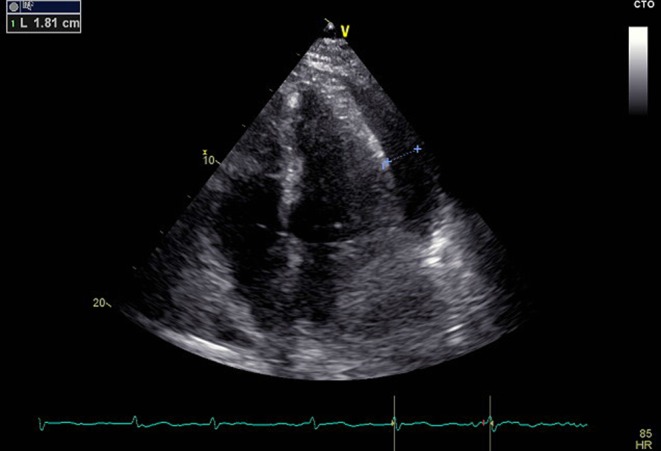
We describe a case of a 40-year-old woman who was admitted to the intensive care unit with a rapid onset of dyspnea and orthopnea. She presented progressive weakness, weight loss and secondary amenorrhea during last year, while intermittent fever was present for the last two months. Initial biochemical evaluation showed anemia, hyponatremia and increased C-reactive protein levels. Clinical and echocardiographic evaluation revealed cardiac tamponade, which was treated with pericardiocentesis. Pleural fluid samples were negative for malignancy, tuberculosis or bacterial infection. Hormonal and serologic evaluation led to the diagnosis of autoimmune polyglandular syndrome (APS) type 2 (including primary adrenal insufficiency and autoimmune thyroiditis), possibly coexisting with systemic lupus erythematosus. After symptomatic rheumatologic treatment followed by replacement therapy with hydrocortisone and fludrocortisone, the patient fully recovered. In patients with the combination of polyserositis, cardiac tamponade and persistent hyponatremia, possible coexistence of rheumatologic and autoimmune endocrine disease, mainly adrenal insufficiency, should be considered. Early diagnosis and non-invasive treatment can be life-saving.
In patients with the combination of polyserositis, cardiac tamponade and persistent hyponatremia, possible coexistence of rheumatologic and autoimmune endocrine disease, mainly adrenal insufficiency, should be considered.Early diagnosis and non-invasive treatment can be life-saving for these patients.Primary adrenal insufficiency requires lifelong replacement therapy with oral administration of 15-25 mg hydrocortisone in split doses and 50-200 µg fludrocortisone once daily.
我们描述了一例40岁女性患者,她因迅速出现的呼吸困难和端坐呼吸入住重症监护病房。她在过去一年中出现进行性虚弱、体重减轻和继发性闭经,在过去两个月中伴有间歇性发热。初始生化评估显示贫血、低钠血症和C反应蛋白水平升高。临床和超声心动图评估显示心包填塞,通过心包穿刺术进行治疗。胸腔积液样本恶性肿瘤、结核或细菌感染检测均为阴性。激素和血清学评估导致诊断为2型自身免疫性多腺体综合征(APS)(包括原发性肾上腺功能不全和自身免疫性甲状腺炎),可能与系统性红斑狼疮共存。经过对症风湿治疗,随后使用氢化可的松和氟氢可的松进行替代治疗后,患者完全康复。对于有多浆膜炎、心包填塞和持续性低钠血症的患者,应考虑风湿性和自身免疫性内分泌疾病(主要是肾上腺功能不全)可能共存。早期诊断和非侵入性治疗可能挽救生命。
对于有多浆膜炎、心包填塞和持续性低钠血症的患者,应考虑风湿性和自身免疫性内分泌疾病(主要是肾上腺功能不全)可能共存。早期诊断和非侵入性治疗对这些患者可能挽救生命。原发性肾上腺功能不全需要终身替代治疗,口服氢化可的松15 - 25毫克,分剂量服用,氟氢可的松50 - 200微克,每日一次。