Tang Zengwei, Yang Yuan, Meng Wenbo, Li Xun
The First Clinical Medical School of Lanzhou University Department of Special Minimally Invasive Surgery, The First Hospital of Lanzhou University The second department of General Surgery, The First Hospital of Lanzhou University, Lanzhou, China Clinical Medical College Cancer Center of Lanzhou University, Lanzhou, China.
Medicine (Baltimore). 2017 Oct;96(43):e8372. doi: 10.1097/MD.0000000000008372.
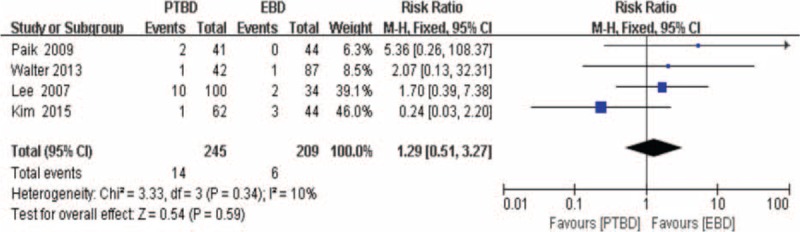
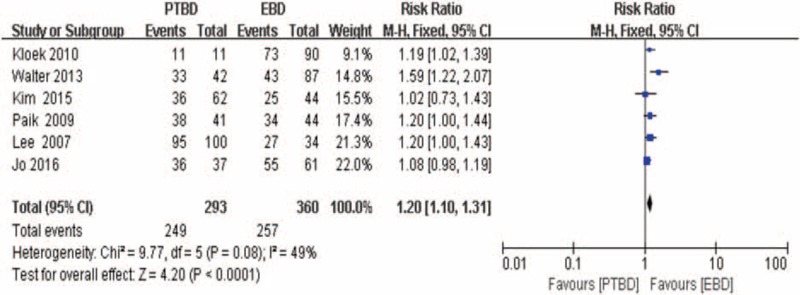
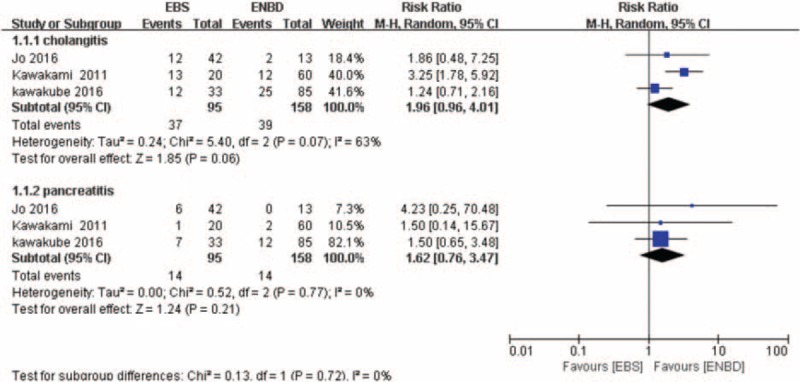
The operative treatment combined with preoperative biliary drainage (PBD) has been established as a safe Klatskin tumor (KT) treatment strategy. However, there has always been a dispute for the preferred technique for PBD technique. This meta-analysis was conducted to compare the biliary drainage-related cholangitis, pancreatitis, hemorrhage, and the success rates of palliative relief of cholestasis between percutaneous transhepatic biliary drainage (PTBD) and endoscopic biliary drainage (EBD), to identify the best technique in the management of KT.PubMed, EMBASE, and Web of Science were searched systematically for prospective or retrospective studies reporting the biliary drainage-related cholangitis, pancreatitis, hemorrhage, and the success rates of palliative relief of cholestasis in patients with KT. A meta-analysis was performed, using the fixed or random-effect model, with Review Manager 5.3.PTBD was associated with lower risk of cholangitis (risk ratio [RR] = 0.49, 95% confidence interval [CI]: 0.36-0.67; P < .00001), particularly in patients with Bismuth-Corlette type II, III, IV KT (RR = 0.50, 95% CI: 0.33-0.77; P = .05). Compared with EBD, PTBD was also associated with a lower risk of pancreatitis (RR = 0.35, 95% CI: 0.17-0.69; P = 0.003) and with higher successful rates of palliative relief of cholestasis (RR = 1.20, 95% CI: 1.10-1.31; P < .0001). The incidence of hemorrhage was similar in these 2 groups (RR 1.29, 95% CI: 0.51-3.27; P = .59). The risk of biliary drainage-related cholangitis (RR = 1.96, 95% CI: 0.96-4.01; P = .06) and pancreatitis (RR = 1.62, 95% CI: 0.76-3.47; P = .21) was similar between endoscopic nasobiliary drainage groups and biliary stenting.In patients with type II or type III or IV KT who need to have PBD, PTBD should be performed as an initial method of biliary drainage in terms of reducing the incidence of procedure related cholangitis, pancreatitis, and improving the rates of palliative relief of cholestasis. Well-conducted randomized controlled trials with a universial criterion for PBD are required to confirm these findings.
手术治疗联合术前胆道引流(PBD)已被确立为一种安全的肝门部胆管癌(KT)治疗策略。然而,对于PBD技术的首选方法一直存在争议。本荟萃分析旨在比较经皮经肝胆道引流(PTBD)和内镜下胆道引流(EBD)在与胆道引流相关的胆管炎、胰腺炎、出血以及胆汁淤积姑息性缓解成功率方面的差异,以确定KT治疗中的最佳技术。
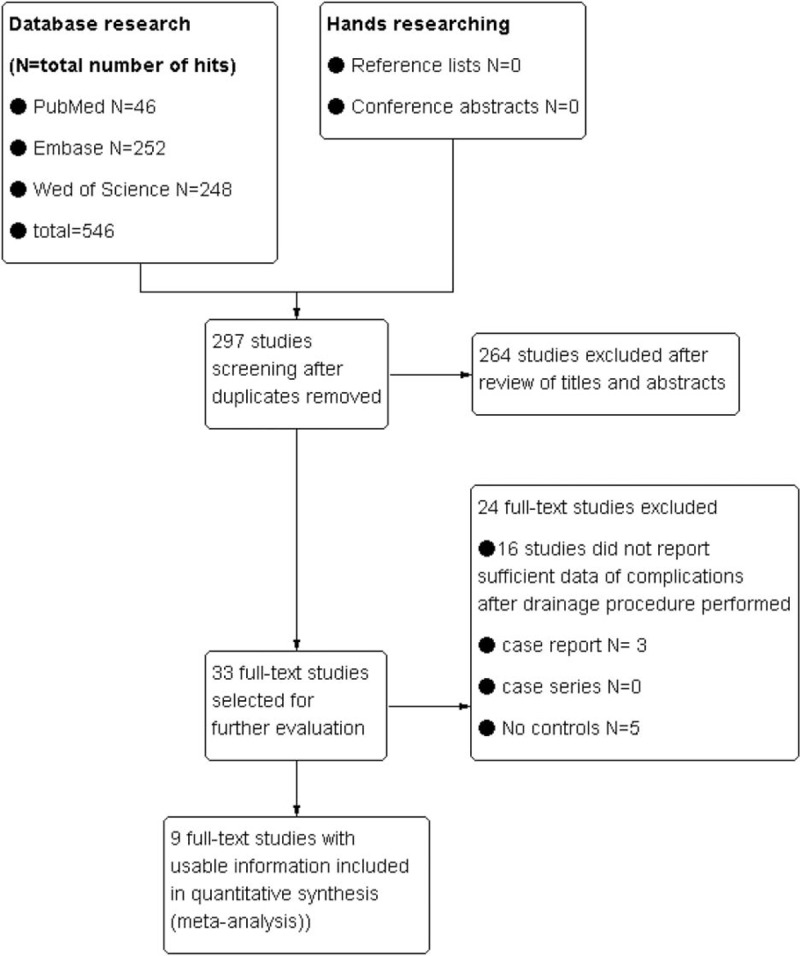
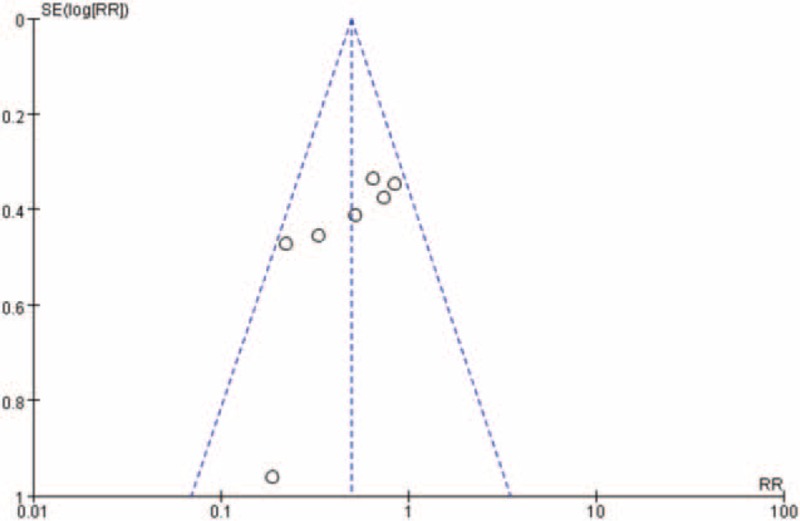
系统检索了PubMed、EMBASE和Web of Science,以查找报告KT患者与胆道引流相关的胆管炎、胰腺炎、出血以及胆汁淤积姑息性缓解成功率的前瞻性或回顾性研究。使用Review Manager 5.3进行荟萃分析,采用固定效应或随机效应模型。
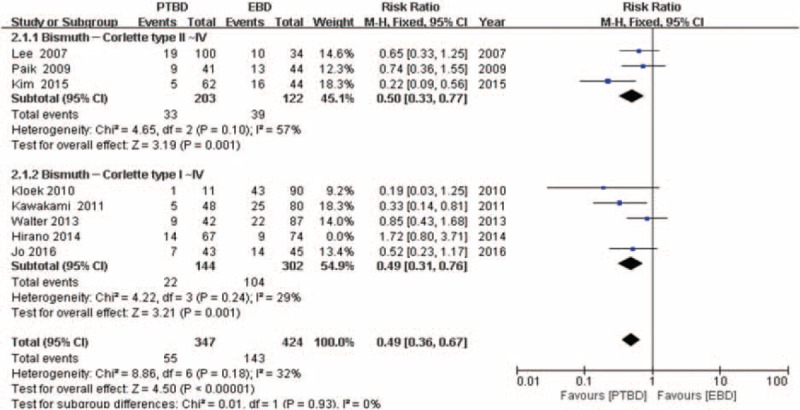
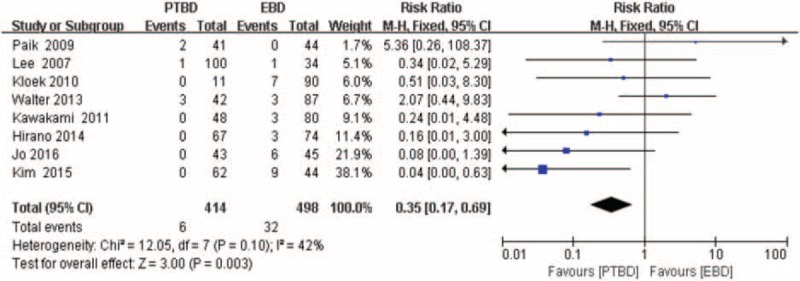
PTBD与较低的胆管炎风险相关(风险比[RR]=0.49,95%置信区间[CI]:0.36 - 0.67;P<.00001),特别是在Bismuth - Corlette II、III、IV型KT患者中(RR=0.50,95% CI:0.33 - 0.77;P=.05)。与EBD相比,PTBD还与较低的胰腺炎风险相关(RR=0.35,95% CI:0.17 - 0.69;P=0.003)以及较高的胆汁淤积姑息性缓解成功率相关(RR=1.20,95% CI:1.10 - 1.31;P<.0001)。两组的出血发生率相似(RR 1.29,95% CI:0.51 - 3.27;P=.59)。内镜鼻胆管引流组和胆道支架置入组在与胆道引流相关的胆管炎(RR=1.96,95% CI:0.96 - 4.01;P=.06)和胰腺炎(RR=1.62,95% CI:0.76 - 3.47;P=.21)风险方面相似。
对于需要进行PBD的II型或III型或IV型KT患者,就降低与手术相关的胆管炎、胰腺炎发生率以及提高胆汁淤积姑息性缓解率而言,PTBD应作为胆道引流的初始方法。需要进行具有通用PBD标准的高质量随机对照试验来证实这些发现。