Department of Plastic and Reconstructive Surgery, Composite Tissue Allotransplantation Immunology Laboratory, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Seongnam, South Korea.
J Transl Med. 2017 Oct 26;15(1):218. doi: 10.1186/s12967-017-1322-5.
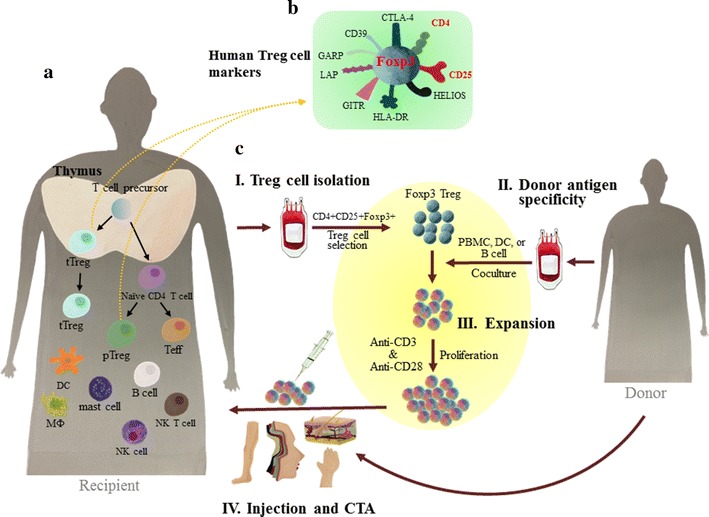
With growing number of cases in recent years, composite tissue allotransplantation (CTA) has been improving the quality of life of patient who seeks reconstruction and repair of damaged tissues. Composite tissue allografts are heterogeneous. They are composed of a variety of tissue types, including skin, muscle, vessel, bone, bone marrow, lymph nodes, nerve, and tendon. As a primary target of CTA, skin has high antigenicity with a rich repertoire of resident cells that play pivotal roles in immune surveillance. In this regard, understanding the molecular mechanisms involved in immune rejection in the skin would be essential to achieve successful CTA. Although scientific evidence has proved the necessity of immunosuppressive drugs to prevent rejection of allotransplanted tissues, there remains a lingering dilemma due to the lack of specificity of targeted immunosuppression and risks of side effects. A cumulative body of evidence has demonstrated T regulatory (Treg) cells have critical roles in induction of immune tolerance and immune homeostasis in preclinical and clinical studies. Presently, controlling immune susceptible characteristics of CTA with adoptive transfer of Treg cells is being considered promising and it has drawn great interests. This updated review will focus on a dominant form of Treg cells expressing CD4CD25 surface molecules and a forkhead box P3 transcription factor with immune tolerant and immune homeostasis activities. For future application of Treg cells as therapeutics in CTA, molecular and cellular characteristics of CTA and immune rejection, Treg cell development and phenotypes, Treg cell plasticity and stability, immune tolerant functions of Treg cells in CTA in preclinical studies, and protocols for therapeutic application of Treg cells in clinical settings are addressed in this review. Collectively, Treg cell therapy in CTA seems feasible with promising perspectives. However, the extreme high immunogenicity of CTA warrants caution.
近年来,随着病例数量的增加,复合组织同种异体移植(CTA)提高了寻求受损组织重建和修复的患者的生活质量。复合组织同种移植物是异质的。它们由多种组织类型组成,包括皮肤、肌肉、血管、骨骼、骨髓、淋巴结、神经和肌腱。作为 CTA 的主要靶标,皮肤具有高抗原性,其中含有丰富的固有细胞,这些细胞在免疫监视中起着关键作用。在这方面,了解皮肤中免疫排斥反应涉及的分子机制对于实现成功的 CTA 至关重要。尽管科学证据已经证明了免疫抑制药物对于防止同种异体移植组织排斥的必要性,但由于靶向免疫抑制缺乏特异性以及副作用的风险,仍然存在一个挥之不去的困境。大量证据表明,调节性 T 细胞(Treg 细胞)在临床前和临床研究中对诱导免疫耐受和免疫稳态具有关键作用。目前,通过过继转移 Treg 细胞来控制 CTA 的免疫敏感性特征被认为是有前途的,并且引起了极大的兴趣。本综述将重点关注表达 CD4CD25 表面分子和叉头框 P3 转录因子的 Treg 细胞的主要形式,这些细胞具有免疫耐受和免疫稳态活性。为了将来将 Treg 细胞作为治疗剂应用于 CTA,本综述还讨论了 CTA 和免疫排斥、Treg 细胞发育和表型、Treg 细胞可塑性和稳定性、Treg 细胞在 CTA 中的免疫耐受功能、以及 Treg 细胞在临床环境中的治疗应用方案等方面的 CTA 分子和细胞特征。总的来说,在 CTA 中进行 Treg 细胞治疗似乎是可行的,具有广阔的前景。然而,CTA 极高的免疫原性需要谨慎对待。