Institut Universitaire de Cardiologie et de Pneumologie de Québec/Québec Heart & Lung Institute Laval University, Québec City, Québec, Canada.
Institut Universitaire de Cardiologie et de Pneumologie de Québec/Québec Heart & Lung Institute Laval University, Québec City, Québec, Canada
J Am Heart Assoc. 2017 Oct 27;6(11):e006309. doi: 10.1161/JAHA.117.006309.
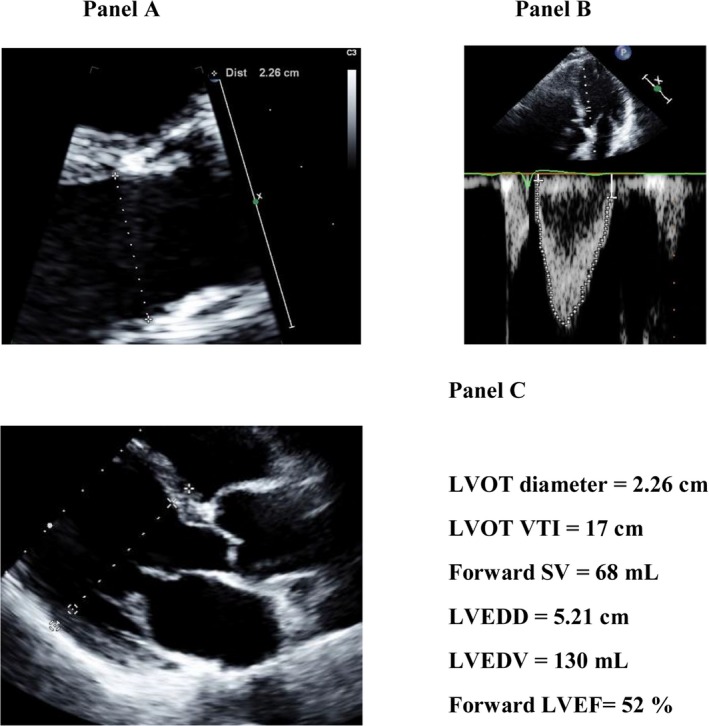
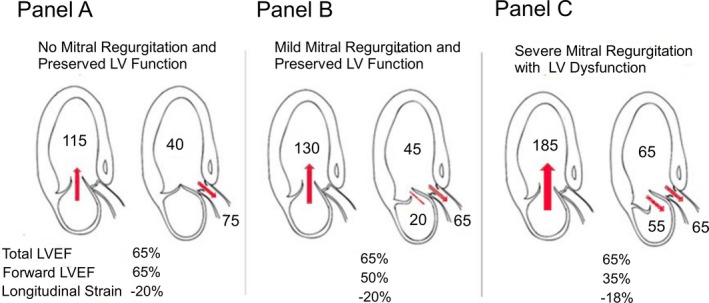
The timing of mitral valve surgery in asymptomatic patients with primary mitral regurgitation (MR) is controversial. We hypothesized that the forward left ventricular (LV) ejection fraction (LVEF; ie, LV outflow tract stroke volume divided by LV end-diastolic volume) is superior to the total LVEF to predict outcomes in MR. The objective of this study was to examine the association between echocardiographic parameters of MR severity and LV function and outcomes in patients with MR.
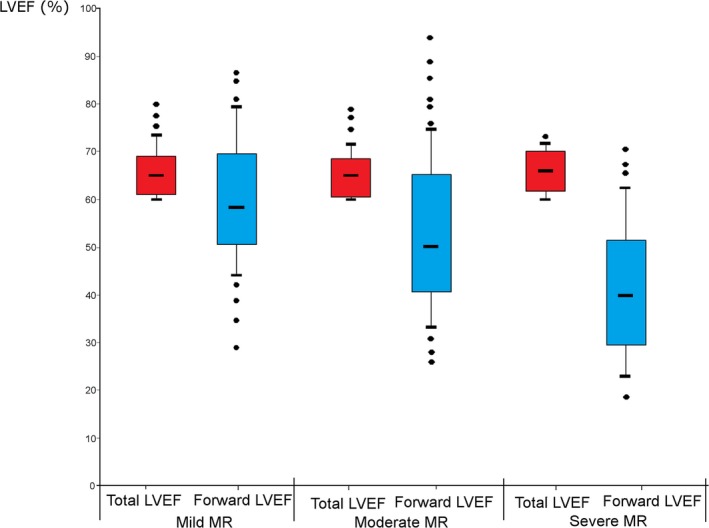
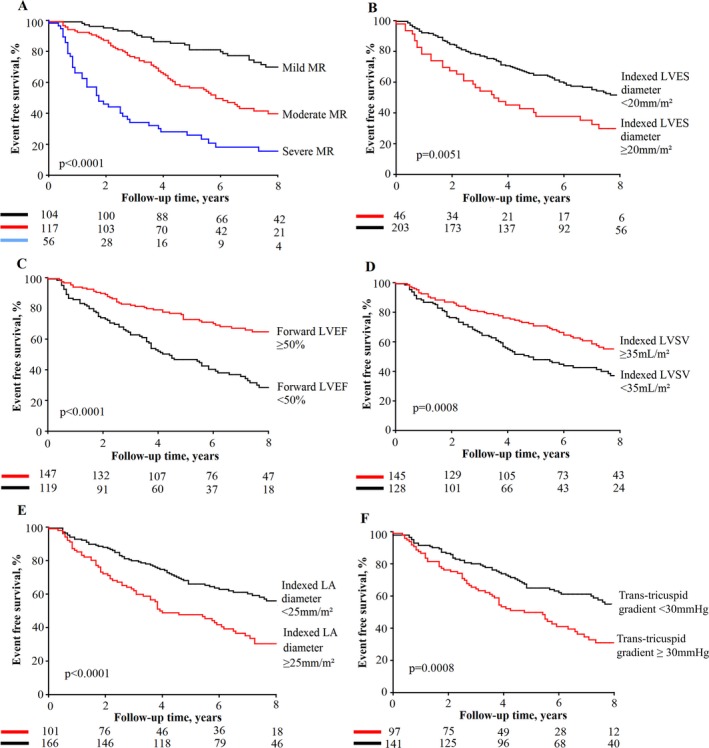
The clinical and Doppler-echocardiographic data of 278 patients with ≥mild MR and no class I indication of mitral valve surgery at baseline were retrospectively analyzed. The primary study end point was the composite of mitral valve surgery or death. During a mean follow-up of 5.4±3.2 years, there were 147 (53%) events: 96 (35%) MV surgeries and 66 (24%) deaths. Total LVEF and global longitudinal strain were not associated with the occurrence of events, whereas forward LVEF (<0.0001) and LV end-systolic diameter (=0.0003) were. After adjustment for age, sex, MR severity, Charlson probability, coronary artery disease, and atrial fibrillation, forward LVEF remained independently associated with the occurrence of events (adjusted hazard ratio: 1.09, [95% confidence interval]: 1.02-1.17 per 5% decrease; =0.01), whereas LV end-systolic diameter was not (=0.48).
The results of this study suggest that the forward LVEF may be superior to the total LVEF and LV end-systolic diameter to predict outcomes in patients with primary MR. This simple and easily measurable parameter may be useful to improve risk stratification and select the best timing for intervention in patients with primary MR.
无症状的原发性二尖瓣反流(MR)患者行二尖瓣手术的时机存在争议。我们假设,左心室(LV)射血分数(LVEF;即 LV 流出道的 stroke volume 除以 LV 舒张末期容积)优于总 LVEF,可预测 MR 患者的结局。本研究旨在探讨 MR 严重程度和 LV 功能的超声心动图参数与 MR 患者结局之间的关系。
回顾性分析了 278 例基线时至少存在中度 MR 且无二尖瓣手术 I 类适应证的患者的临床和多普勒超声心动图数据。主要研究终点是复合终点,包括二尖瓣手术或死亡。平均随访 5.4±3.2 年后,发生了 147 例(53%)事件:96 例(35%)行 MV 手术,66 例(24%)死亡。总 LVEF 和整体纵向应变与事件的发生无关,而前向 LVEF(<0.0001)和 LV 收缩末期直径(=0.0003)则有关。在校正年龄、性别、MR 严重程度、Charlson 概率、冠状动脉疾病和心房颤动后,前向 LVEF 仍然与事件的发生独立相关(调整后的危险比:每降低 5%,为 1.09[95%置信区间:1.02-1.17];=0.01),而 LV 收缩末期直径则无关(=0.48)。
本研究结果表明,前向 LVEF 可能优于总 LVEF 和 LV 收缩末期直径,可预测原发性 MR 患者的结局。这种简单且易于测量的参数可能有助于改善风险分层,并为原发性 MR 患者选择最佳干预时机。