University of Calgary, Calgary, AB, Canada
Alberta Health, Edmonton, AB, Canada.
J Am Heart Assoc. 2017 Oct 28;6(11):e007129. doi: 10.1161/JAHA.117.007129.
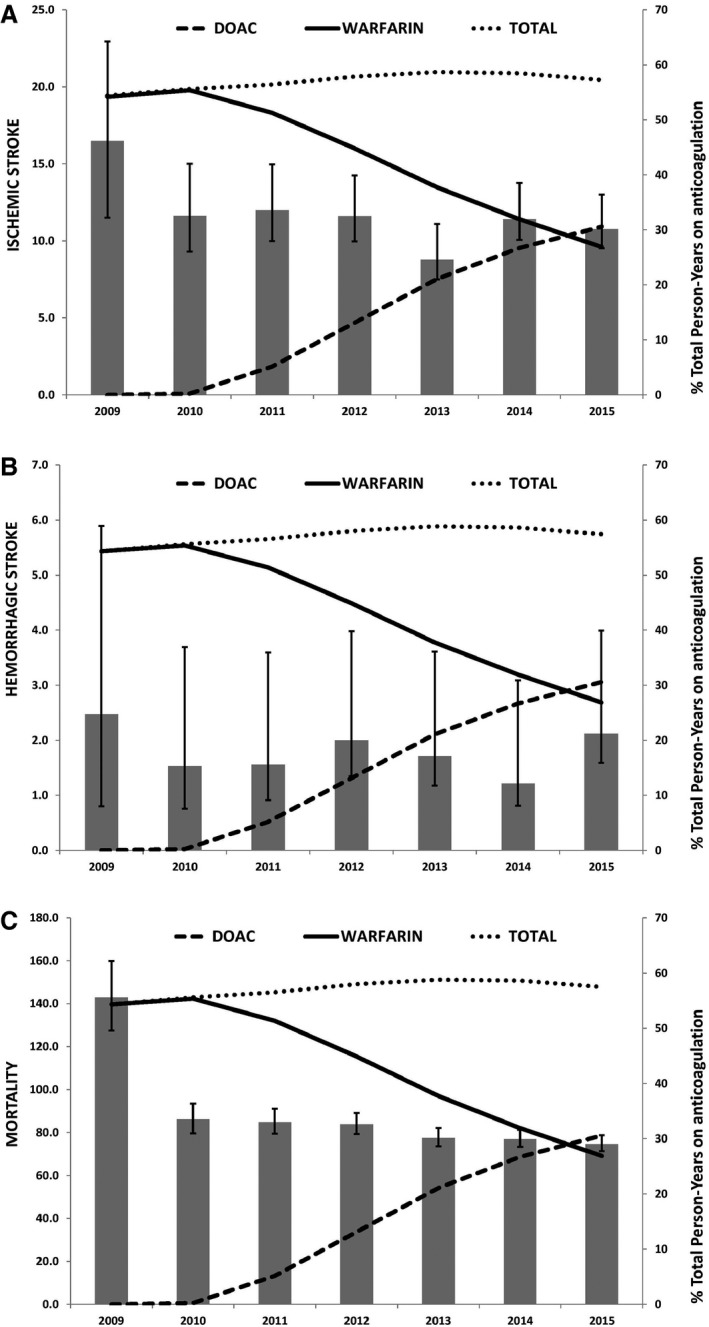
Direct oral anticoagulants (DOACs) are noninferior to warfarin for stroke prevention in atrial fibrillation (AF). We aimed to determine the population risk of stroke and death in incident AF, stratified by anticoagulation status and type, and the temporal trends of oral anticoagulation practice in the post-DOAC approval period.
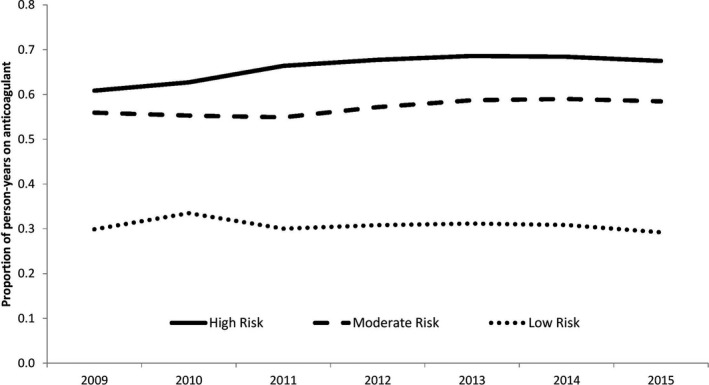
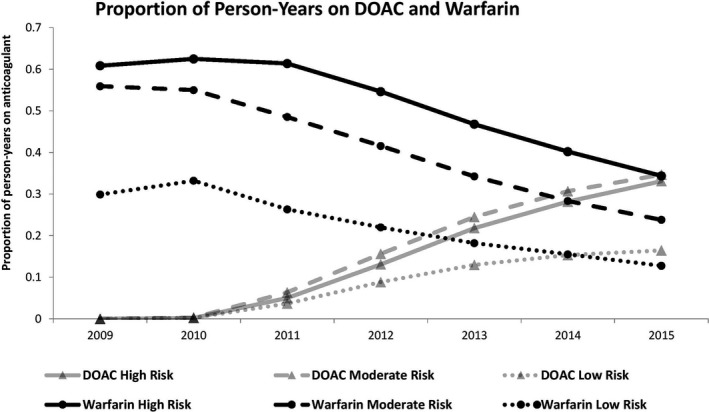
We conducted a population-based cohort study of incident nonvalvular AF cases using administrative health data in Alberta, Canada. We used Cox proportional hazards modeling with anticoagulation status as a time-varying exposure and adjusted for age (continuous), sex, congestive heart failure, hypertension, diabetes mellitus, prior transient ischemic attack or ischemic stroke, myocardial infarction, peripheral artery disease, and chronic kidney disease. Primary outcome was the composite of stroke and death. Among 34 965 patients with incident AF (56.0% male, median age 73 years), relative to warfarin, DOAC use was associated with decreased risk of all stroke and death (hazard ratio: 0.90; 95% confidence interval, 0.83-0.97) and decreased hemorrhagic stroke (hazard ratio: 0.60; 95% confidence interval, 0.40-0.91]) but a similar risk of ischemic stroke (hazard ratio: 1.12; 95% confidence interval, 0.94-1.34]). During this time period, DOAC use increased rapidly, surpassing warfarin, but the total oral anticoagulation use in the population remained stable, even in the subgroup with the highest thromboembolic risk.
In a real-world population-based study of patients with incident AF, anticoagulation with DOACs was associated with decreased risk of stroke and death compared with warfarin. Despite a rapid uptake of DOACs in clinical practice, the total proportion of AF patients on anticoagulation has remained stable, even in high-risk patients.
直接口服抗凝剂(DOAC)在预防房颤(AF)中的卒中发生方面不劣于华法林。我们旨在确定 AF 患者中按抗凝状态和类型分层的卒中与死亡的人群风险,并确定 DOAC 批准后时期口服抗凝治疗的时间趋势。
我们使用加拿大艾伯塔省的行政健康数据进行了一项基于人群的非瓣膜性 AF 病例队列研究。我们使用 Cox 比例风险模型,将抗凝状态作为时变暴露,并调整年龄(连续)、性别、充血性心力衰竭、高血压、糖尿病、短暂性脑缺血发作或缺血性卒中、心肌梗死、外周动脉疾病和慢性肾脏病。主要结局是卒中与死亡的复合结局。在 34965 例新发 AF 患者(56.0%为男性,中位年龄 73 岁)中,与华法林相比,DOAC 治疗与所有卒中与死亡风险降低相关(风险比:0.90;95%置信区间,0.83-0.97),与出血性卒中风险降低相关(风险比:0.60;95%置信区间,0.40-0.91),但缺血性卒中风险相似(风险比:1.12;95%置信区间,0.94-1.34)。在此期间,DOAC 的使用迅速增加,超过了华法林,但人群中总的口服抗凝治疗仍保持稳定,即使在血栓栓塞风险最高的亚组中也是如此。
在一项基于真实世界的新发 AF 患者人群研究中,与华法林相比,DOAC 抗凝治疗与卒中与死亡风险降低相关。尽管 DOAC 在临床实践中的应用迅速增加,但 AF 患者接受抗凝治疗的总比例保持稳定,即使在高危患者中也是如此。