Yao Xiaoxi, Abraham Neena S, Sangaralingham Lindsey R, Bellolio M Fernanda, McBane Robert D, Shah Nilay D, Noseworthy Peter A
Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery, Mayo Clinic, Rochester, MN Division of Health Care Policy and Research, Department of Health Sciences Research, Mayo Clinic, Rochester, MN
Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery, Mayo Clinic, Rochester, MN Division of Health Care Policy and Research, Department of Health Sciences Research, Mayo Clinic, Rochester, MN Division of Gastroenterology and Hepatology, Department of Medicine, Mayo Clinic, Scottsdale, AZ.
J Am Heart Assoc. 2016 Jun 13;5(6):e003725. doi: 10.1161/JAHA.116.003725.
The introduction of non-vitamin K antagonist oral anticoagulants has been a major advance for stroke prevention in atrial fibrillation; however, outcomes achieved in clinical trials may not translate to routine practice. We aimed to evaluate the effectiveness and safety of dabigatran, rivaroxaban, and apixaban by comparing each agent with warfarin.
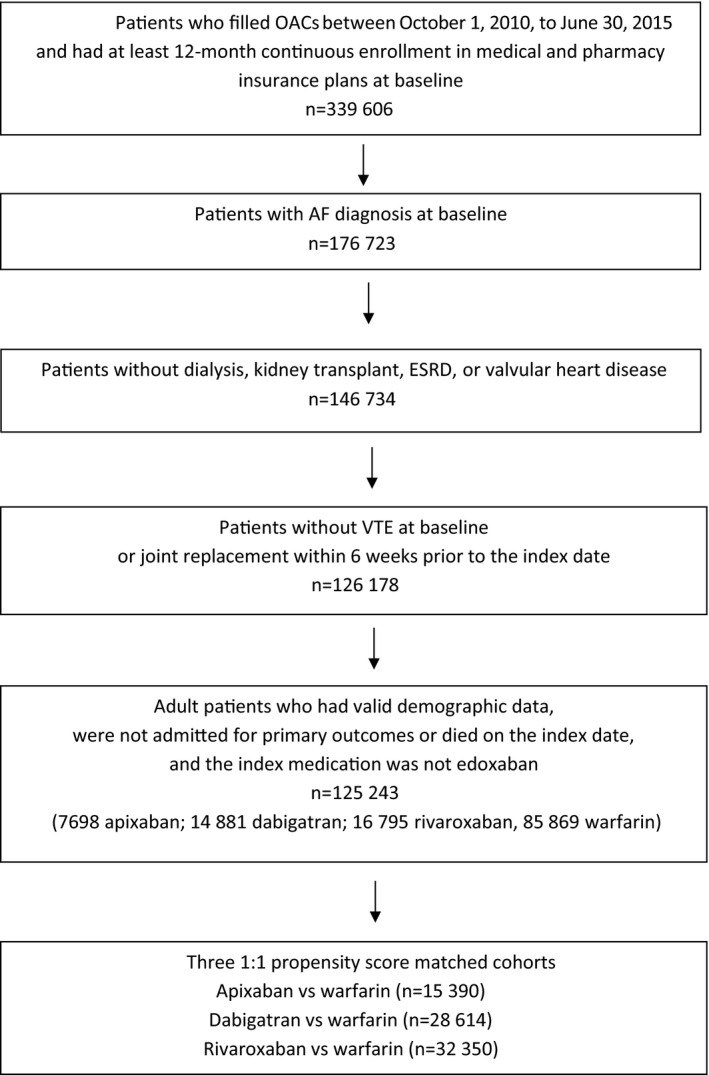
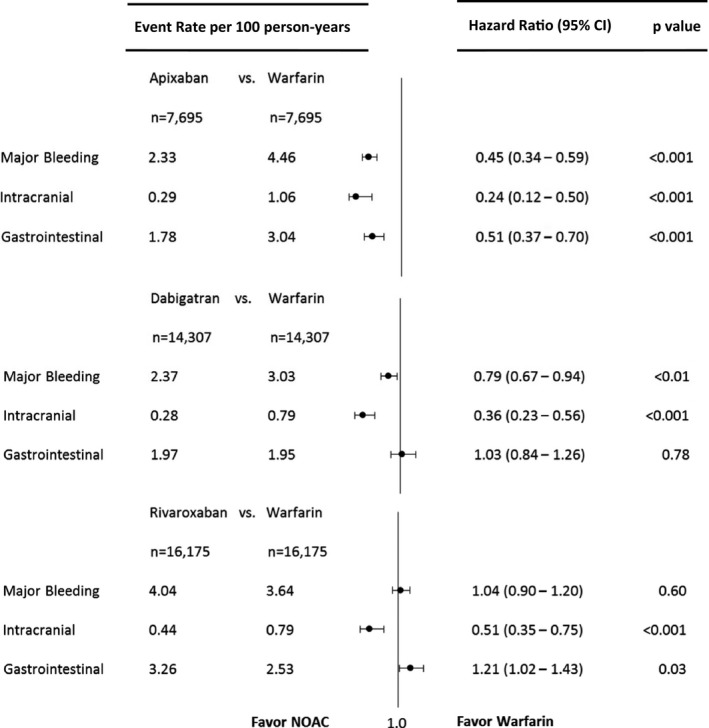
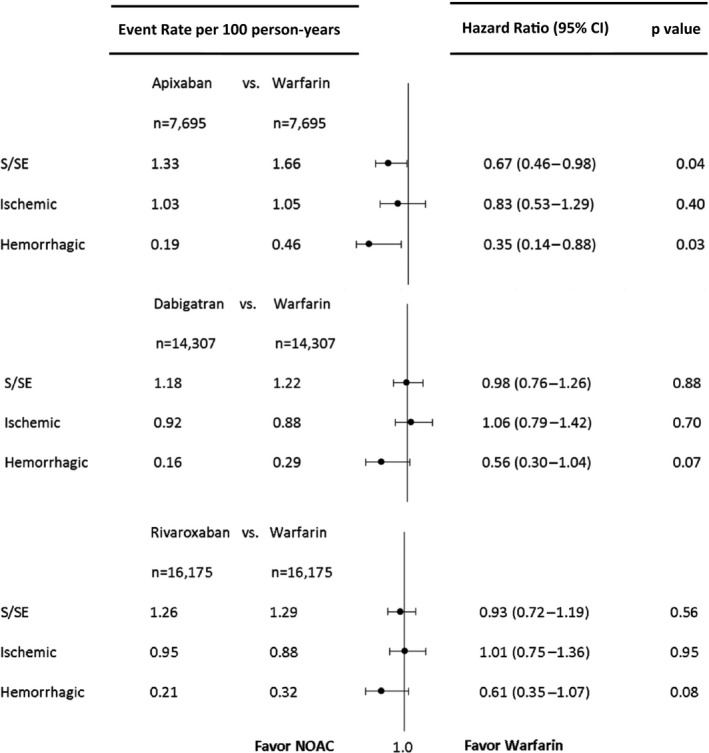
Using a large US insurance database, we identified privately insured and Medicare Advantage patients with nonvalvular atrial fibrillation who were users of apixaban, dabigatran, rivaroxaban, or warfarin between October 1, 2010, and June 30, 2015. We created 3 matched cohorts using 1:1 propensity score matching: apixaban versus warfarin (n=15 390), dabigatran versus warfarin (n=28 614), and rivaroxaban versus warfarin (n=32 350). Using Cox proportional hazards regression, we found that for stroke or systemic embolism, apixaban was associated with lower risk (hazard ratio [HR] 0.67, 95% CI 0.46-0.98, P=0.04), but dabigatran and rivaroxaban were associated with a similar risk (dabigatran: HR 0.98, 95% CI 0.76-1.26, P=0.98; rivaroxaban: HR 0.93, 95% CI 0.72-1.19, P=0.56). For major bleeding, apixaban and dabigatran were associated with lower risk (apixaban: HR 0.45, 95% CI 0.34-0.59, P<0.001; dabigatran: HR 0.79, 95% CI 0.67-0.94, P<0.01), and rivaroxaban was associated with a similar risk (HR 1.04, 95% CI 0.90-1.20], P=0.60). All non-vitamin K antagonist oral anticoagulants were associated with a lower risk of intracranial bleeding.
In patients with nonvalvular atrial fibrillation, apixaban was associated with lower risks of both stroke and major bleeding, dabigatran was associated with similar risk of stroke but lower risk of major bleeding, and rivaroxaban was associated with similar risks of both stroke and major bleeding in comparison to warfarin.
非维生素K拮抗剂口服抗凝药的引入是心房颤动卒中预防领域的一项重大进展;然而,临床试验取得的结果可能无法转化为常规实践。我们旨在通过比较达比加群、利伐沙班和阿哌沙班与华法林,评估它们的有效性和安全性。
利用美国一个大型保险数据库,我们确定了2010年10月1日至2015年6月30日期间使用阿哌沙班、达比加群、利伐沙班或华法林的非瓣膜性心房颤动的私人保险和医疗保险优势患者。我们使用1:1倾向评分匹配创建了3个匹配队列:阿哌沙班与华法林(n = 15390)、达比加群与华法林(n = 28614)、利伐沙班与华法林(n = 32350)。使用Cox比例风险回归,我们发现,对于卒中或全身性栓塞,阿哌沙班的风险较低(风险比[HR] 0.67,95%CI 0.46 - 0.98,P = 0.04),但达比加群和利伐沙班的风险相似(达比加群:HR 0.98,95%CI 0.76 - 1.26,P = 0.98;利伐沙班:HR 0.93,95%CI 0.72 - 1.19,P = 0.56)。对于大出血,阿哌沙班和达比加群的风险较低(阿哌沙班:HR 0.45,95%CI 0.34 - 0.59,P < 0.001;达比加群:HR 0.79,95%CI 0.67 - 0.94,P < 0.01),利伐沙班的风险相似(HR 1.04,95%CI 0.90 - 1.20,P = 0.60)。所有非维生素K拮抗剂口服抗凝药的颅内出血风险均较低。
在非瓣膜性心房颤动患者中,与华法林相比,阿哌沙班的卒中和大出血风险均较低,达比加群的卒中风险相似但大出血风险较低,利伐沙班的卒中和大出血风险相似。