Medicine, University of Birmingham, Birmingham, UK.
Medical Student, Health Sciences University of Mongolia, Ulaanbaatar, Mongolia.
Int J Equity Health. 2017 Oct 30;16(1):189. doi: 10.1186/s12939-017-0684-x.
To understand the effect of economic growth on health, we investigated the trend in socio-economic and regional determinants of child health in Mongolia. This Central Asian country had the fastest economic growth amongst low and middle-income countries (LMICs) from 2000 to 2010 and a healthcare system in transition.
Data was from Mongolian multiple indicator cluster surveys (MICS) in 2000, 2005 and 2010. Child nutrition/growth was measured by height-for-age z-score (HAZ), weight-for-age z-score (WAZ), prevalence of stunted (HAZ < -2) and underweight (WAZ < -2) children. Access to health care was measured by prevalence of fully immunised children <5 years. Multivariate multi-level logistic mixed modelling was used to estimate the effect of socio-economic and environmental health determinants on each outcome in each year; 2000, 2005 and 2010. T-tests were used to measure significant change in HAZ and WAZ over the decade.
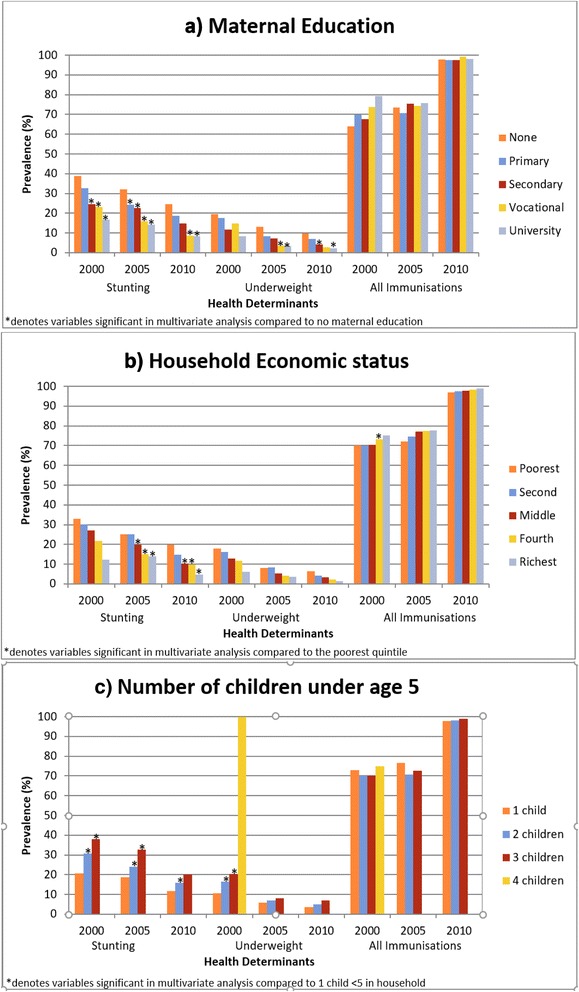
Overall, from 2000 to 2010, there was a significant improvement (p < 0.001) in all three outcomes, but the effect of socio-economic factors increased on both stunting and weight. In 2000, region was a significant determinant: children living in three provinces were significantly more likely to be stunted and less likely to be immunised than Ulaanbaatar, but this was not significant by 2010. By 2010, none of the factors were significant determinants of immunisation in children. In 2000, economic status had no effect on stunting (OR = 0.91; 95%CI:0.49,1.66), however by 2010, children in the poorest economic quintile were 4 times more likely to be stunted than the richest (OR = 0.24; 95% CI:0.13,0.45; p < 0.001). The effect of maternal education on stunting prevalence continued over the 10 years, in both 2000 and 2010 children were twice as likely to be stunted if their mother had no education compared to university education (2000 OR = 0.45; 95% CI:0.28,0.73, p < 0.01,2010 OR =0.55; 95% CI:0.35,0.87, p < 0.05).
Economic growth in Mongolia from 2000 to 2010 resulted in an increase in the effect of social determinants of child health; whilst focused policy improved access to immunisation. Children with less educated mothers and lower household incomes should be targeted in interventions to reduce health inequity.
为了了解经济增长对健康的影响,我们调查了蒙古儿童健康的社会经济和地区决定因素的趋势。作为中亚国家,蒙古在 2000 年至 2010 年间是中低收入国家中经济增长最快的国家,其医疗保健系统也在转型。
数据来自蒙古的多次指标群集调查(MICS),时间为 2000 年、2005 年和 2010 年。儿童营养/生长通过身高年龄 Z 分数(HAZ)、体重年龄 Z 分数(WAZ)来衡量,包括发育迟缓(HAZ <-2)和体重不足(WAZ <-2)儿童的患病率。通过 5 岁以下完全免疫儿童的患病率来衡量获得医疗保健的情况。使用多变量多水平逻辑混合模型来估计 2000 年、2005 年和 2010 年每个年份社会经济和环境卫生决定因素对每个结果的影响;使用 t 检验来衡量过去十年 HAZ 和 WAZ 的显著变化。
总体而言,从 2000 年到 2010 年,所有三个结果都有显著改善(p < 0.001),但社会经济因素对发育迟缓的影响以及体重的影响都有所增加。2000 年,地区是一个重要的决定因素:与乌兰巴托相比,生活在三个省份的儿童发育迟缓的可能性显著更高,而接受免疫接种的可能性显著更低,但到 2010 年,这一情况不再显著。到 2010 年,没有任何因素是儿童免疫接种的重要决定因素。2000 年,经济状况对发育迟缓没有影响(OR = 0.91;95%CI:0.49,1.66),但到 2010 年,最贫困的五分之一家庭的儿童发育迟缓的可能性是最富裕家庭的四倍(OR = 0.24;95%CI:0.13,0.45;p < 0.001)。母亲教育对发育迟缓患病率的影响在过去 10 年中持续存在,与接受过大学教育的儿童相比,母亲没有接受过教育的儿童发育迟缓的可能性是其两倍(2000 年 OR = 0.45;95%CI:0.28,0.73,p < 0.01,2010 年 OR = 0.55;95%CI:0.35,0.87,p < 0.05)。
2000 年至 2010 年蒙古的经济增长导致儿童健康的社会决定因素的影响增加;而重点政策改善了免疫接种的可及性。应该针对母亲教育程度较低和家庭收入较低的儿童开展干预措施,以减少健康不平等。