Wang Hong-De, Li Tong, Gao Shi-Jun
Department of Orthopedics, The Third Hospital of Hebei Medical University, 139 Ziqiang Road, Shijiazhuang, 050051, Hebei, People's Republic of China.
Orthopaedic Biomechanics Laboratory of Hebei Province, 139 Ziqiang Road, Shijiazhuang, 050051, Hebei, People's Republic of China.
J Orthop Surg Res. 2017 Oct 30;12(1):161. doi: 10.1186/s13018-017-0661-5.
Discoid medial meniscus is an extremely rare abnormality of the knee. During arthroscopic meniscectomy for symptomatic discoid medial meniscus, it is difficult to remove the posterior portion of the meniscus because of the confined working space within the compartment and the obstruction caused by the anterior cruciate ligament and the tibial intercondylar eminence. To overcome these problems, we describe an improved arthroscopic technique for one-piece excision of symptomatic discoid medial meniscus through three unique portals.
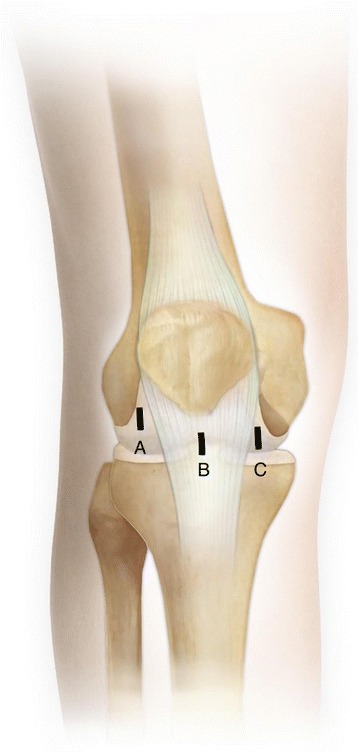
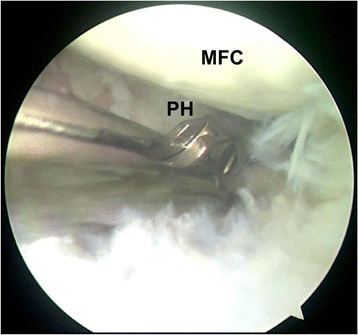
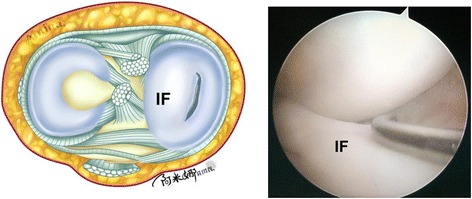
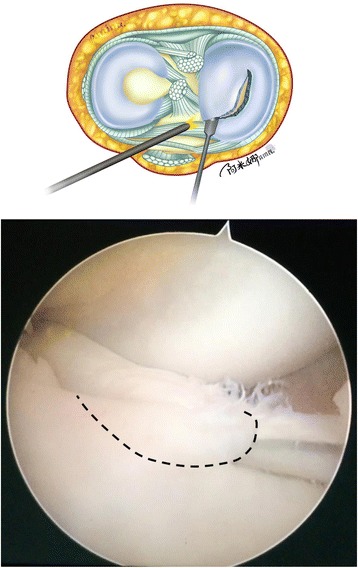
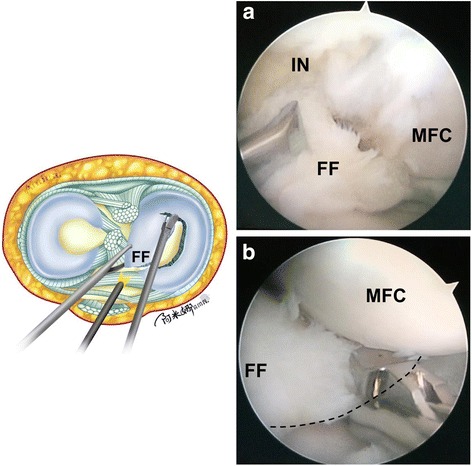
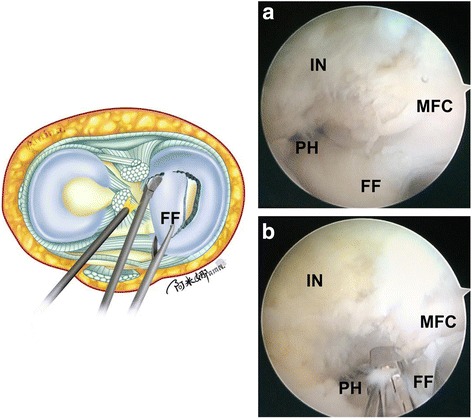
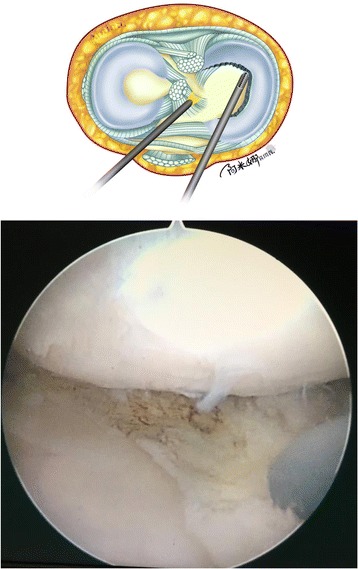
Three improved portals were made in the injured knee: a standard anteromedial portal, a central transpatellar tendon portal, and a high anterolateral portal. The anterior side of the discoid medial meniscus was cut 7 mm from the periphery of the meniscus. Next, the anterior portion of the free discoid meniscus fragment was pulled in the anterolateral direction with tension. A curve-shaped cut was made along the longitudinal tear to the posterior horn using basket forceps through the standard anteromedial portal. Then, the anterior portion of the free discoid meniscus was pulled in the anteromedial direction. Pulling the fragment under tension made it easier to cut the posterior side of the discoid meniscus. The posterior side of the discoid meniscus was cut 7 mm from the periphery of the meniscus with straight scissors or basket forceps through the central transpatellar tendon portal.
This technique resulted in satisfactory results. Excellent visualization of the posterior part of the discoid medial meniscus was gained during the procedure, and it was easy to cut the posterior part of the discoid medial meniscus. No recurrent symptoms were found.
This improved arthroscopic one-piece excision technique for the treatment of symptomatic discoid medial meniscus enables the posterior part of the meniscus to be cut satisfactorily. Moreover, compared with previous techniques, this novel technique causes less formation of foreign bodies and less damage to the anterior cruciate ligament, medial collateral ligament, and cartilage and requires a shorter procedural time.
盘状内侧半月板是一种极其罕见的膝关节异常。在对有症状的盘状内侧半月板进行关节镜下半月板切除术时,由于关节间隙内工作空间有限以及前交叉韧带和胫骨髁间隆起造成的阻碍,很难切除半月板的后部。为克服这些问题,我们描述一种通过三个独特切口进行有症状盘状内侧半月板整块切除的改良关节镜技术。
在受伤膝关节处制作三个改良切口:一个标准前内侧切口、一个经髌腱中央切口和一个高位前外侧切口。从半月板边缘向内侧7毫米处切开盘状内侧半月板的前侧。接着,将游离的盘状半月板碎片的前部向外侧方向牵拉并施加张力。使用篮钳通过标准前内侧切口沿着纵向撕裂口向后角制作一条曲线形切口。然后,将游离的盘状半月板前部向内侧方向牵拉。在张力下牵拉碎片便于切除盘状半月板的后侧。通过经髌腱中央切口用直剪刀或篮钳从半月板边缘向内侧7毫米处切开盘状半月板的后侧。
该技术取得了满意的效果。术中对盘状内侧半月板后部有极佳的视野,并且很容易切除盘状内侧半月板的后部。未发现复发症状。
这种改良的关节镜下整块切除技术用于治疗有症状的盘状内侧半月板能够令人满意地切除半月板后部。此外,与先前技术相比,这种新技术产生的异物形成较少,对前交叉韧带、内侧副韧带和软骨的损伤较小,且手术时间更短。