Cross J Helen, Auvin Stéphane, Falip Mercè, Striano Pasquale, Arzimanoglou Alexis
Clinical Neurosciences Section, UCL Institute of Child Health, ERN EpiCARE, London, United Kingdom.
APHP, Robert Debré University Hospital, Paris, France.
Front Neurol. 2017 Sep 29;8:505. doi: 10.3389/fneur.2017.00505. eCollection 2017.
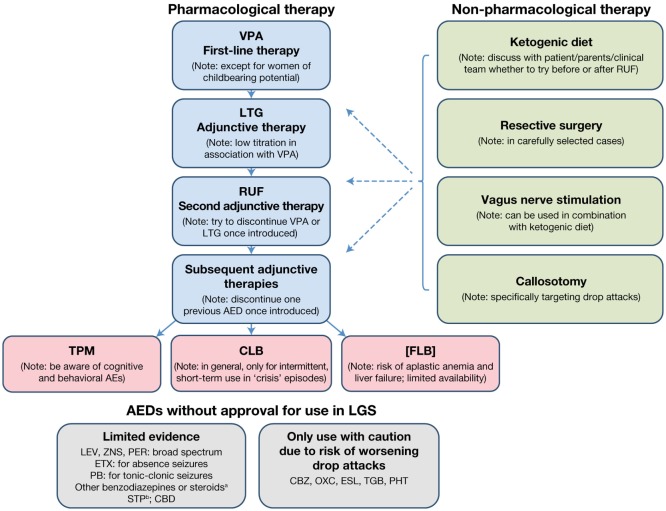
Lennox-Gastaut syndrome (LGS) is a severe epileptic and developmental encephalopathy that is associated with a high rate of morbidity and mortality. It is characterized by multiple seizure types, abnormal electroencephalographic features, and intellectual disability. Although intellectual disability and associated behavioral problems are characteristic of LGS, they are not necessarily present at its outset and are therefore not part of its diagnostic criteria. LGS is typically treated with a variety of pharmacological and non-pharmacological therapies, often in combination. Management and treatment decisions can be challenging, due to the multiple seizure types and comorbidities associated with the condition. A panel of five epileptologists met to discuss consensus recommendations for LGS management, based on the latest available evidence from literature review and clinical experience. Treatment algorithms were formulated. Current evidence favors the continued use of sodium valproate (VPA) as the first-line treatment for patients with newly diagnosed LGS. If VPA is ineffective alone, evidence supports lamotrigine, or subsequently rufinamide, as adjunctive therapy. If seizure control remains inadequate, the choice of next adjunctive antiepileptic drug (AED) should be discussed with the patient/parent/caregiver/clinical team, as current evidence is limited. Non-pharmacological therapies, including resective surgery, the ketogenic diet, vagus nerve stimulation, and callosotomy, should be considered for use alongside AED therapy from the outset of treatment. For patients with LGS that has evolved from another type of epilepsy who are already being treated with an AED other than VPA, VPA therapy should be considered if not trialed previously. Thereafter, the approach for a patient should be followed. Where possible, no more than two AEDs should be used concomitantly. Patients with established LGS should undergo review by a neurologist specialized in epilepsy on at least an annual basis, including a thorough reassessment of their diagnosis and treatment plan. Clinicians should always be vigilant to the possibility of treatable etiologies and alert to the possibility that a patient's diagnosis may change, since the seizure types and electroencephalographic features that characterize LGS evolve over time. To date, available treatments are unlikely to lead to seizure remission in the majority of patients and therefore the primary focus of treatment should always be optimization of learning, behavioral management, and overall quality of life.
Lennox-Gastaut综合征(LGS)是一种严重的癫痫性和发育性脑病,其发病率和死亡率很高。它的特征是多种发作类型、异常脑电图特征和智力残疾。虽然智力残疾和相关行为问题是LGS的特征,但它们不一定在疾病开始时就出现,因此不是其诊断标准的一部分。LGS通常采用多种药物和非药物疗法进行治疗,通常联合使用。由于与该疾病相关的多种发作类型和合并症,管理和治疗决策可能具有挑战性。一个由五名癫痫专家组成的小组开会讨论了基于文献综述和临床经验的最新可用证据制定的LGS管理共识建议。制定了治疗算法。目前的证据支持继续使用丙戊酸钠(VPA)作为新诊断LGS患者的一线治疗药物。如果VPA单独无效,证据支持拉莫三嗪或随后的卢非酰胺作为辅助治疗。如果癫痫控制仍然不足,由于目前证据有限,应与患者/家长/护理人员/临床团队讨论下一种辅助抗癫痫药物(AED)的选择。从治疗开始就应考虑将包括切除性手术、生酮饮食、迷走神经刺激和胼胝体切开术在内的非药物疗法与AED疗法一起使用。对于已从另一种类型癫痫演变而来且已接受除VPA以外的AED治疗的LGS患者,如果之前未进行过试验,应考虑使用VPA治疗。此后,应遵循针对患者的治疗方法。在可能的情况下,同时使用的AED不应超过两种。确诊LGS的患者应至少每年由专门从事癫痫治疗的神经科医生进行复查,包括对其诊断和治疗计划进行全面重新评估。临床医生应始终警惕可治疗病因的可能性,并警惕患者诊断可能发生变化的可能性,因为LGS的发作类型和脑电图特征会随时间演变。迄今为止,现有的治疗方法不太可能使大多数患者的癫痫发作缓解,因此治疗的主要重点应始终是优化学习、行为管理和整体生活质量。