Zheng Wen, Yu Cheuk-Man, Liu Jing, Xie Wu-Xiang, Wang Miao, Zhang Yu-Jiao, Sun Jian, Nie Shao-Ping, Zhao Dong
Department of Epidemiology, Beijing Anzhen Hospital, Capital Medical University, Beijing Institute of Heart, Lung and Blood Vessel Diseases, No.2 Anzhen Road, Chaoyang District, Beijing, China.
Emergency Critical Care Center, Beijing Anzhen Hospital, Capital Medical University, Beijing, China.
J Geriatr Cardiol. 2017 Aug;14(8):524-531. doi: 10.11909/j.issn.1671-5411.2017.08.006.
There are still a high proportion of patients with ST-segment elevation myocardial infarction (STEMI) missing out early reperfusion even in the primary percutaneous coronary intervention (PCI) era. Most of them are stable latecomers, but the optimal time to undergo delayed PCI for stable ones remains controversial.
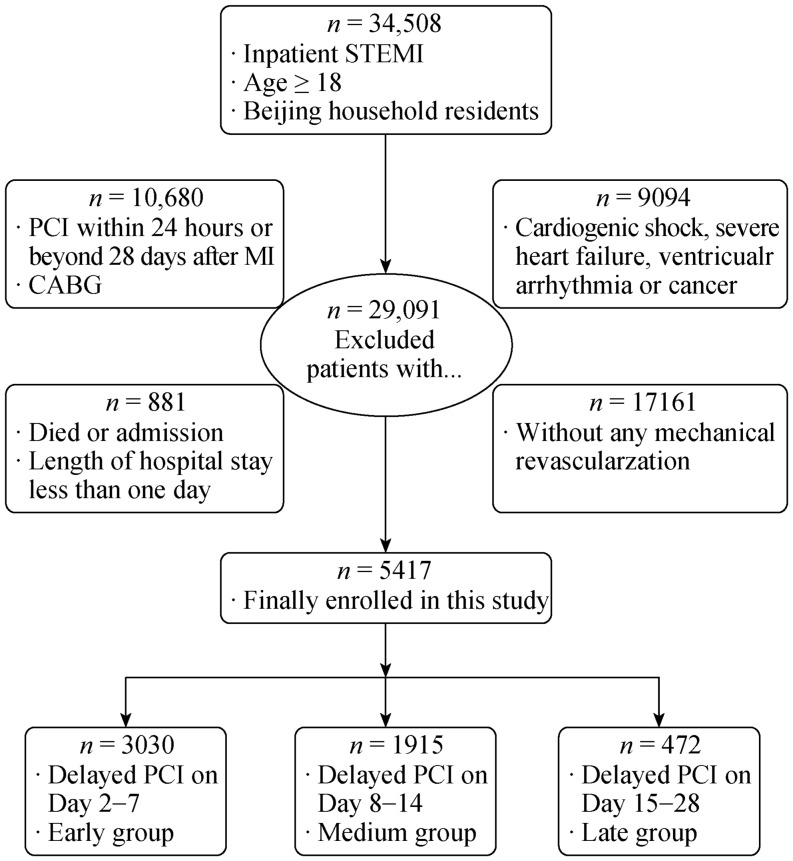
We investigated all STEMI patients who underwent delayed PCI (2-28 days after STEMI) during 2007-2010 in Beijing and excluded patients with hemodynamic instability. The primary outcome was major adverse cardiovascular events (MACEs).
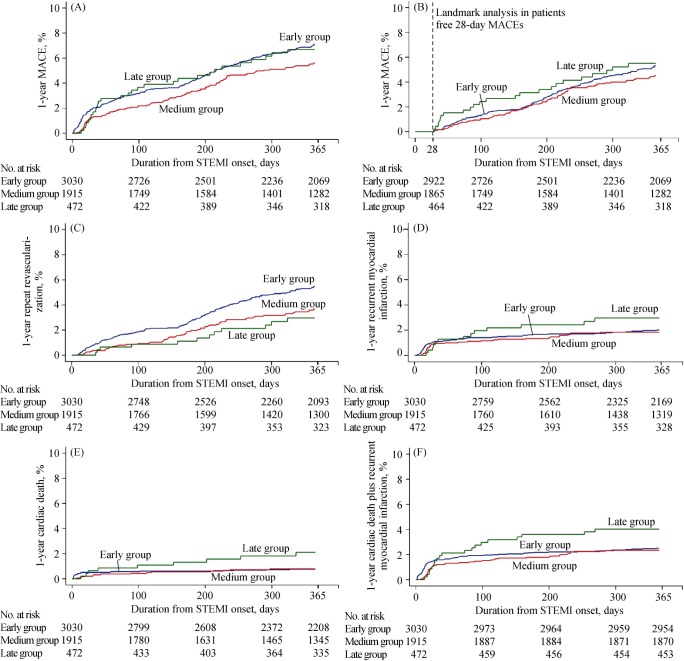
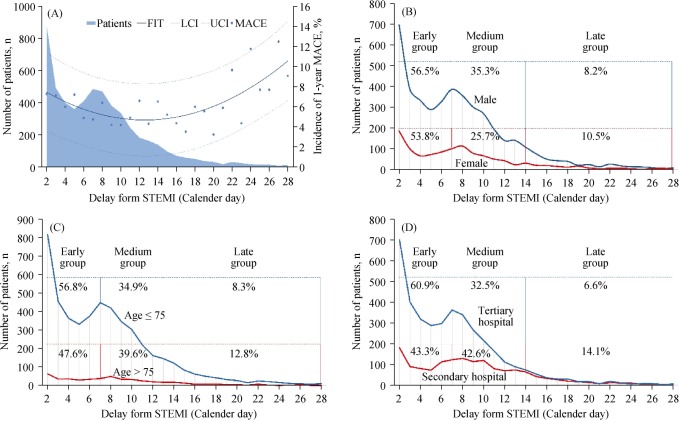
This study finally enrolled 5,417 STEMI patients and assigned them into three groups according to individual delayed time (Early group, 55.9%; Medium group, 35.4%; Late group, 8.7%). During 1-year follow-up, MACEs occurred in 319 patients. The incidence of MACEs were respectively 7.1%, 5.6% and 6.7% among three groups. The Medium group had less recurrent myocardial infarction plus cardiac death (hazard ratio, 0.525; 95% confidence interval, 0.294-0.938, = 0.030) than Late group and less repeat revascularization (hazard ratio, 0.640; 95% confidence interval, 0.463-0.883, = 0.007) than Early group in pairwise comparisons. We depicted the incidence of major adverse cardiovascular event (MACE) by delayed time as a quadratic curve and found the bottom appeared at day 14.
The delayed PCI time varied in the real-world practice, but undergoing operations on the second week after STEMI had greater survival benefit and less adverse events for whom without early reperfusion and hemodynamic instability.
即使在直接经皮冠状动脉介入治疗(PCI)时代,仍有很大比例的ST段抬高型心肌梗死(STEMI)患者未能实现早期再灌注。其中大多数是病情稳定的延迟就诊者,但对于稳定型患者进行延迟PCI的最佳时机仍存在争议。
我们调查了2007年至2010年在北京接受延迟PCI(STEMI后2 - 28天)的所有STEMI患者,并排除了血流动力学不稳定的患者。主要结局是主要不良心血管事件(MACE)。
本研究最终纳入了5417例STEMI患者,并根据个体延迟时间将他们分为三组(早期组,55.9%;中期组,35.4%;晚期组,8.7%)。在1年的随访期间,319例患者发生了MACE。三组中MACE的发生率分别为7.1%、5.6%和6.7%。在两两比较中,中期组复发性心肌梗死加心源性死亡的发生率低于晚期组(风险比,0.525;95%置信区间,0.294 - 0.938,P = 0.030),重复血运重建的发生率低于早期组(风险比,0.640;95%置信区间,0.463 - 0.883,P = 0.007)。我们将主要不良心血管事件(MACE)的发生率按延迟时间描绘为一条二次曲线,发现最低点出现在第14天。
在实际临床实践中,延迟PCI的时间各不相同,但对于那些没有早期再灌注且血流动力学稳定的STEMI患者,在STEMI后第二周进行手术具有更大的生存获益和更少的不良事件。