Bayliss Elizabeth A, Reifler Liza M, Zeng Chan, McQuillan Deanna B, Ellis Jennifer L, Steiner John F
Institute for Health Research, Kaiser Permanente Colorado, Denver, CO, USA.
J Comorb. 2014 Aug 18;4:29-36. doi: 10.15256/joc.2014.4.41. eCollection 2014.
Cancer patients with cardiovascular and other comorbidities are at concurrent risk of multiple adverse outcomes. However, most treatment decisions are guided by evidence from single-outcome models, which may be misleading for multimorbid patients.
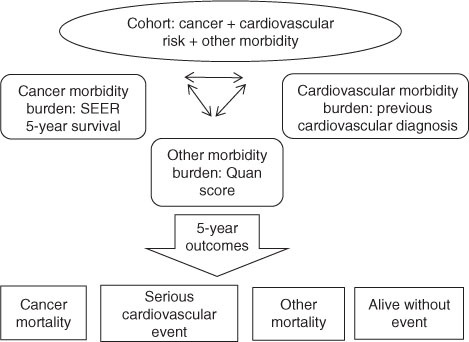
We assessed the interacting effects of cancer, cardiovascular, and other morbidity burdens on the competing outcomes of cancer mortality, serious cardiovascular events, and other-cause mortality.
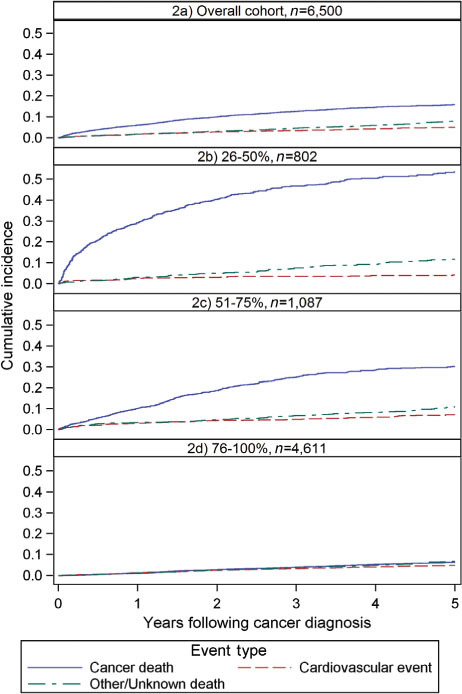
We analyzed a cohort of 6,500 adults with initial cancer diagnosis between 2001 and 2008, SEER 5-year survival ≥26%, and a range of cardiovascular risk factors. We estimated the cumulative incidence of cancer mortality, a serious cardiovascular event (myocardial infarction, coronary revascularization, or cardiovascular mortality), and other-cause mortality over 5 years, and identified factors associated with the competing risks of each outcome using cause-specific Cox proportional hazard models.
Following cancer diagnosis, there were 996 (15.3%) cancer deaths, 328 (5.1%) serious cardiovascular events, and 542 (8.3%) deaths from other causes. In all, 4,634 (71.3%) cohort members had none of these outcomes. Although cancer prognosis had the greatest effect, cardiovascular and other morbidity also independently increased the hazard of each outcome. The effect of cancer prognosis on outcome was greatest in year 1, and the effect of other morbidity was greater in individuals with better cancer prognoses.
In multimorbid oncology populations, comorbidities interact to affect the competing risk of different outcomes. Quantifying these risks may provide persons with cancer plus cardiovascular and other comorbidities more accurate information for shared decision-making than risks calculated from single-outcome models. Journal of Comorbidity 2014;4:29-36.
患有心血管疾病及其他合并症的癌症患者同时面临多种不良后果的风险。然而,大多数治疗决策是基于单结局模型的证据,这对于患有多种疾病的患者可能具有误导性。
我们评估了癌症、心血管疾病和其他疾病负担对癌症死亡率、严重心血管事件和其他原因死亡率等相互竞争结局的交互作用。
我们分析了一组6500名成年人,他们在2001年至2008年间首次被诊断患有癌症,监测、流行病学和最终结果(SEER)5年生存率≥26%,且存在一系列心血管危险因素。我们估计了5年内癌症死亡率、严重心血管事件(心肌梗死、冠状动脉血运重建或心血管疾病死亡率)和其他原因死亡率的累积发生率,并使用特定病因的Cox比例风险模型确定与每个结局的竞争风险相关的因素。
癌症诊断后,有996例(15.3%)癌症死亡,328例(5.1%)严重心血管事件,542例(8.3%)其他原因死亡。总共有4634例(71.3%)队列成员未出现这些结局。尽管癌症预后的影响最大,但心血管疾病和其他疾病也独立增加了每个结局的风险。癌症预后对结局的影响在第1年最大,其他疾病的影响在癌症预后较好的个体中更大。
在患有多种疾病的肿瘤患者群体中,合并症相互作用以影响不同结局的竞争风险。与单结局模型计算的风险相比,量化这些风险可能为患有癌症以及心血管疾病和其他合并症的患者提供更准确的信息,以便进行共同决策。《合并症杂志》2014年;4:29 - 36。