Čačala Sharon R, Gilart José
All authors: Grey's Hospital, University of KwaZulu-Natal, Pietermaritzburg, South Africa.
J Glob Oncol. 2017 Mar 8;3(5):497-501. doi: 10.1200/JGO.2016.008060. eCollection 2017 Oct.
Patients with breast cancer (BC) in Area 2 KwaZulu-Natal, South Africa, often present with advanced disease. We performed a review of the patients' sociodemographic characteristics and their reasons for late presentation to identify what changes could be made to improve time to presentation.
Fifty women with T1, T2, T3, or T4 BC were assessed for sociodemographic data. Patients in T3 and T4 groups were asked to provide reasons for late presentation.
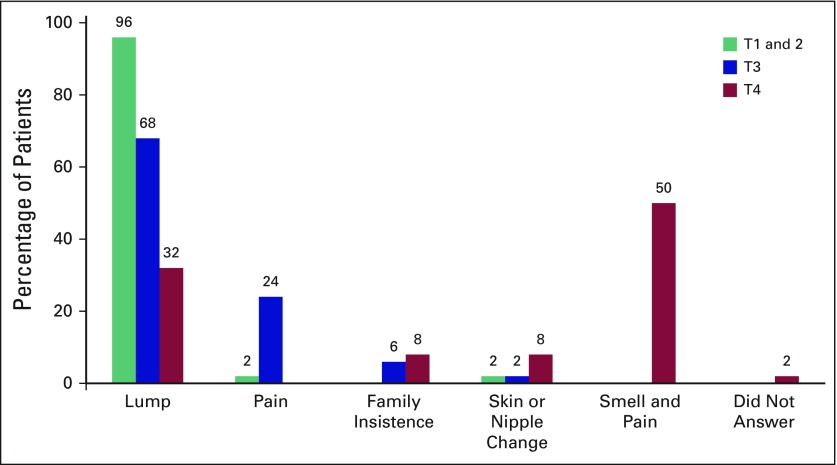
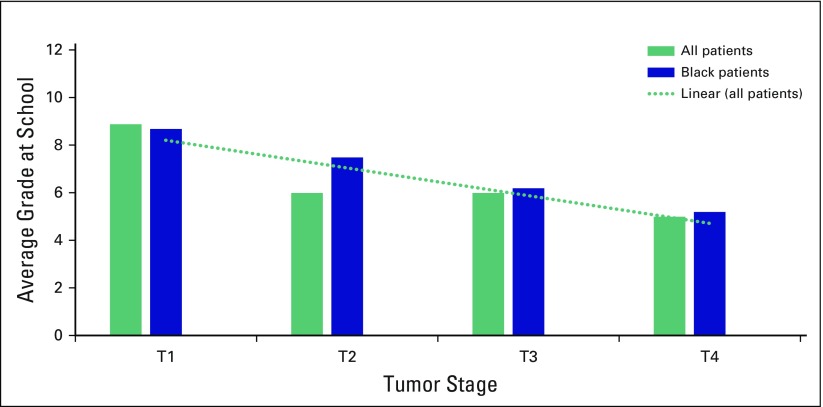
Of 172 patients, 50 had T2, T3, or T4 BC, and 22 had T1. Age ranged from 23 to 100 years (average, 56 years). There was no significant difference in age for different tumor sizes. The average size of a T1 tumor was 1.8 cm; T2, 3.6 cm; T3, 11.4 cm; and T4, 14.8 cm. Regarding education, 19% of patients had never attended school (T1, 5%; T2, 12%; T3, 22%; T4, 32%), and 19% had completed their education (finished 12th grade). The average education level was 6th grade. Patients with larger tumors had less education ( < .05). Of the patients who lived in rural areas, 41% had T1, 52% had T2, 66% had T3, and 78% had T4 tumors ( < .01). Patients with larger tumors were associated with having less electricity in their homes than patients with smaller tumors ( < .05). Patients presented with a variety of symptoms. A breast lump was the presenting complaint in 96% of T1 and T2, 68% of T3 and 32% of T4; with a nipple or skin change, 2% of T3 and 8% of T4; because their families insisted, 6% of T3 and 8% of T4; because of pain, 24% of T3; and because of pain with malodorous smell, 50% of T4. Patients' reasons for late presentation were fear (40%), not aware of disease severity (40%), fear of losing a breast (40%), referral problems (34%), financial problems (8%), and transportation problems (6%). Approximately 33% sought medical help from traditional healers, and 65% regularly attended clinics.
Patients who presented late often lived in rural areas with fewer amenities (such as having no electricity in their homes), less education, and poor understanding of BC. Pictorial information about BC needs to be introduced to people who live in rural communities, and opportunistic screening needs to be provided at local clinics.
南非夸祖鲁 - 纳塔尔省2区的乳腺癌患者通常就诊时已处于疾病晚期。我们对患者的社会人口学特征及其就诊延迟的原因进行了回顾,以确定可以做出哪些改变来缩短就诊时间。
对50例患有T1、T2、T3或T4期乳腺癌的女性进行了社会人口学数据评估。T3和T4组的患者被要求提供就诊延迟的原因。
在172例患者中,50例患有T2、T3或T4期乳腺癌,22例患有T1期。年龄范围为23至100岁(平均56岁)。不同肿瘤大小的患者年龄无显著差异。T1期肿瘤的平均大小为1.8厘米;T2期为3.6厘米;T3期为11.4厘米;T4期为14.8厘米。在教育程度方面,19%的患者从未上学(T1期为5%;T2期为12%;T3期为22%;T4期为32%),19%的患者完成了学业(读完12年级)。平均教育水平为6年级。肿瘤较大的患者受教育程度较低(P<0.05)。居住在农村地区的患者中,41%患有T1期肿瘤,52%患有T2期,66%患有T3期,78%患有T4期肿瘤(P<0.01)。与肿瘤较小的患者相比,肿瘤较大的患者家中通电情况较差(P<0.05)。患者表现出多种症状。乳房肿块是96%的T1和T2期、68%的T3期和32%的T4期患者的首发症状;乳头或皮肤改变是2%的T3期和8%的T4期患者的首发症状;因家人坚持就诊的占T3期的6%和T4期的8%;因疼痛就诊的占T3期的24%;因疼痛伴恶臭就诊的占T4期的50%。患者就诊延迟的原因包括恐惧(40%)、未意识到疾病严重性(40%)、害怕失去乳房(40%)、转诊问题(34%)、经济问题(8%)和交通问题(6%)。约33%的患者向传统治疗师寻求医疗帮助,65%的患者定期到诊所就诊。
就诊延迟的患者通常居住在农村地区,生活设施较少(如家中不通电),教育程度较低,对乳腺癌的了解不足。需要向农村社区居民介绍有关乳腺癌的图片信息,并在当地诊所提供机会性筛查。