Department of Radiation Oncology, Memorial Sloan Kettering Cancer Center, New York, NY, USA.
New York University School of Medicine, New York, NY, USA.
Ann Surg Oncol. 2018 Jan;25(1):154-163. doi: 10.1245/s10434-017-6209-4. Epub 2017 Nov 1.
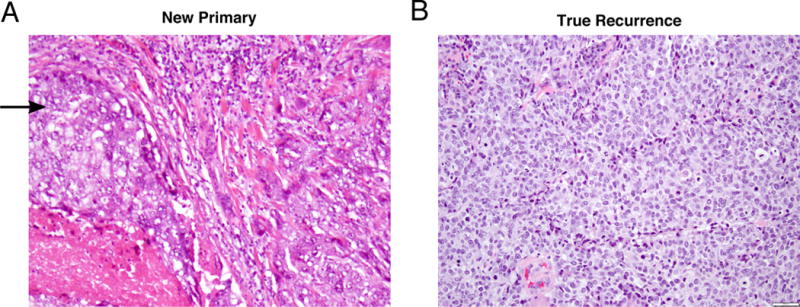
Among all in-breast tumor recurrences (IBTR) following breast-conserving therapy (BCT), some comprise metachronous new primaries (NPs) while others are true recurrences (TRs). Establishing this distinction remains a challenge.
We studied 3932 women who underwent BCT for stage I-III breast cancer from 1998 to 2008. Of these, 115 (2.9%) had an IBTR. Excluding patients with inoperable/unresectable recurrences or simultaneous distant metastases, 81 patients with isolated IBTR comprised the study population. An IBTR was categorized as an NP rather than a TR if it included an in situ component. The log-rank test and Kaplan-Meier method were used to evaluate disease-free survival (DFS) and overall survival (OS), and univariate and multivariate analyses were performed using Cox proportional hazards regression models.
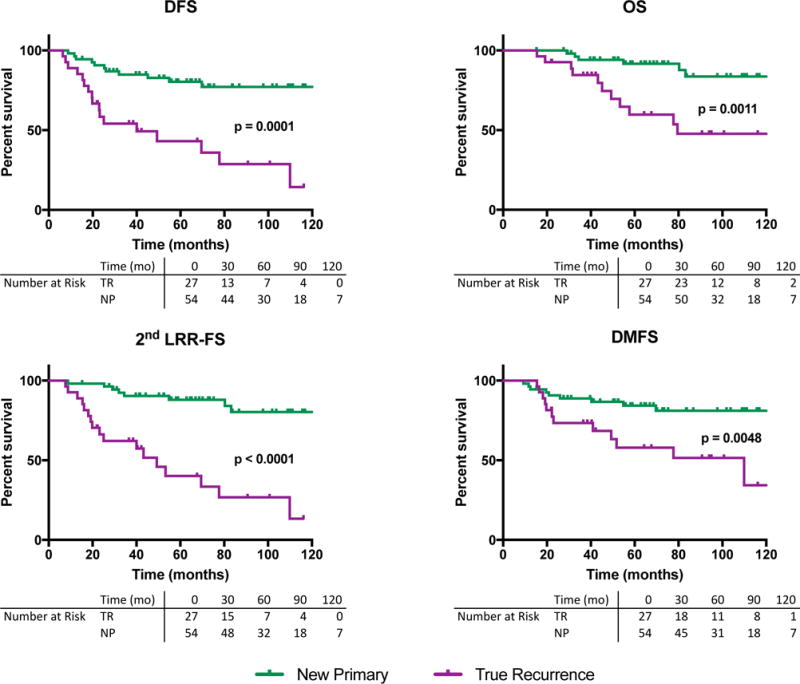
At a median of 64.5 months from IBTR diagnosis, 28 of 81 patients had DFS events. Five-year DFS was 43.1% in the TR group (p = 0.0001) versus 80.3% in the NP group, while 5-year OS was 59.7% in the TR group versus 91.7% among those with NPs (p = 0.0011). On univariate analysis, increasing tumor size, high grade, positive margins, lymphovascular invasion, node involvement, lack of axillary surgery, chemotherapy, radiation therapy, and IBTR type (TR vs. NP) were significantly associated with worse DFS. Controlling for tumor size and margin status, TRs remained significantly associated with lower DFS (hazard ratio 3.717, 95% confidence interval 1.607-8.595, p = 0.002).
The presence of an in situ component is associated with prognosis among patients with IBTR following BCT and may be useful in differentiating TRs and NPs.
在保乳治疗(BCT)后所有的乳房内肿瘤复发(IBTR)中,有些是同时性新原发肿瘤(NPs),而另一些则是真正的复发(TRs)。确定这种区别仍然是一个挑战。
我们研究了 1998 年至 2008 年间接受 I-III 期乳腺癌 BCT 的 3932 名女性。其中 115 名(2.9%)有 IBTR。排除无法手术/不可切除的复发或同时远处转移的患者后,81 名孤立性 IBTR 患者纳入研究人群。如果 IBTR 包括原位成分,则将其归类为 NP 而不是 TR。使用对数秩检验和 Kaplan-Meier 方法评估无病生存率(DFS)和总生存率(OS),并使用 Cox 比例风险回归模型进行单因素和多因素分析。
在从 IBTR 诊断到中位 64.5 个月时,81 名患者中有 28 名发生了 DFS 事件。TR 组的 5 年 DFS 为 43.1%(p=0.0001),而 NP 组为 80.3%,TR 组的 5 年 OS 为 59.7%,而 NP 组为 91.7%(p=0.0011)。单因素分析显示,肿瘤大小增加、高级别、阳性切缘、脉管侵犯、淋巴结受累、缺乏腋窝手术、化疗、放疗以及 IBTR 类型(TR 与 NP)与较差的 DFS 显著相关。控制肿瘤大小和切缘状态后,TR 与较低的 DFS 显著相关(风险比 3.717,95%置信区间 1.607-8.595,p=0.002)。
在 BCT 后 IBTR 患者中,原位成分的存在与预后相关,可能有助于区分 TRs 和 NPs。