Health Center Alte Mälzerei, Regensburg, Germany.
Department Hematology and Oncology, University Hospital Regensburg, Regensburg, Germany.
Med Oncol. 2017 Nov 2;34(12):192. doi: 10.1007/s12032-017-1040-0.
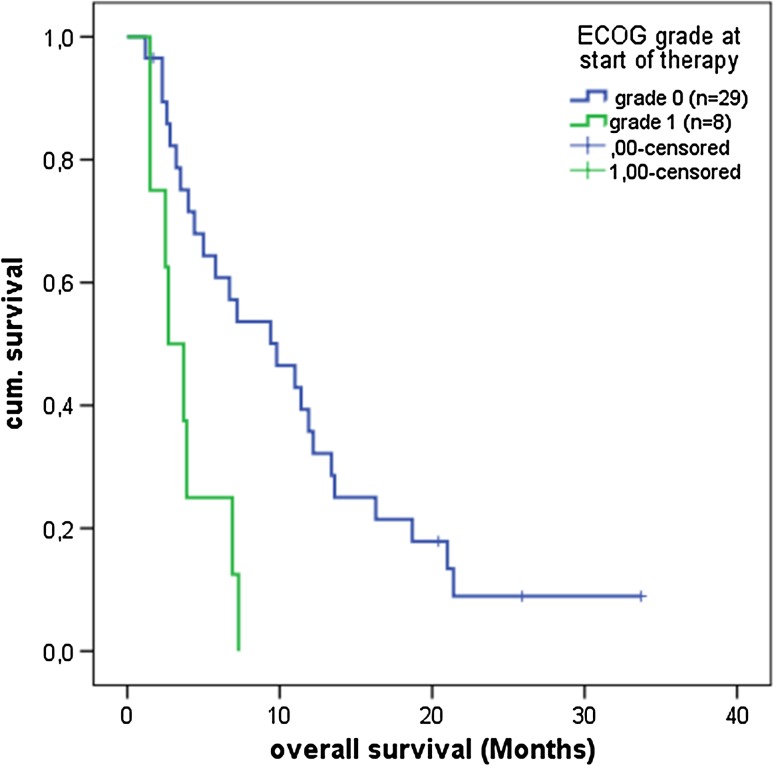
Systemic therapy for advanced hepatocellular carcinoma (HCC) is still challenging. A biomodulatory therapy approach targeting the communicative infrastructure of HCC, including metronomic low-dose chemotherapy with capecitabine, pioglitazone and rofecoxib, has been evaluated in patients with non-curative HCC. Altogether 38 patients were evaluable in this one-arm, multicenter phase II trial. The primary endpoint, median progression-free survival was 2.7 months (95% CI: 1.6-3.79) for all evaluable patients and 8.4 months (95% CI: 0-18.13) for patients ≥ 6 weeks on protocol. Median overall survival (OS) was 6.7 months (95% CI: 4.08-9.31) and 9.4 months (95% CI: 4.82-13.97), respectively. Most common adverse events were edemas grade 3, which were commonly related to the advanced stage, with 66% of the patients suffering from liver cirrhosis. Exploratory data analyses showed significant impact of ECOG performance status grade 0 versus 1 and CLIP score 0/1 versus > 1 on OS, 9.8 months (95% CI: 4.24-15.35) versus 2.7 months (95% CI: 1.03-4.36; P = 0.002), and 9.8 months (95% CI: 3.23-16.37) versus 4.4 months (95% CI: 3.14-5.66; P = 0.009), respectively. Preceding tumor surgery had significant beneficial impact on survival, as well as maximal tumor diameter of < 5 cm. The correlation of C-reactive protein decrease with significantly improved OS underlines the close link between inflammation and tumor control. Biomodulatory therapy in advanced HCC may be a low toxic, efficacious treatment and principally demonstrates that such approaches should be followed further for treatment of advanced HCC.
晚期肝细胞癌(HCC)的系统治疗仍然具有挑战性。针对 HCC 通讯基础设施的生物调节治疗方法,包括卡培他滨、吡格列酮和罗非昔布的低剂量节拍化疗,已在不可治愈的 HCC 患者中进行了评估。在这项单臂、多中心 II 期试验中,共有 38 名患者可评估。主要终点,所有可评估患者的中位无进展生存期为 2.7 个月(95%CI:1.6-3.79),方案治疗≥6 周的患者为 8.4 个月(95%CI:0-18.13)。中位总生存期(OS)分别为 6.7 个月(95%CI:4.08-9.31)和 9.4 个月(95%CI:4.82-13.97)。最常见的不良反应是 3 级水肿,这通常与晚期有关,66%的患者患有肝硬化。探索性数据分析表明,ECOG 表现状态等级 0 与 1 以及 CLIP 评分 0/1 与>1 对 OS 有显著影响,9.8 个月(95%CI:4.24-15.35)与 2.7 个月(95%CI:1.03-4.36;P=0.002),9.8 个月(95%CI:3.23-16.37)与 4.4 个月(95%CI:3.14-5.66;P=0.009)。先前的肿瘤手术对生存有显著的有益影响,最大肿瘤直径<5cm 也是如此。C-反应蛋白下降与 OS 的显著改善相关,强调了炎症与肿瘤控制之间的密切联系。晚期 HCC 的生物调节治疗可能是一种低毒、有效的治疗方法,主要表明此类方法应进一步用于晚期 HCC 的治疗。