Chen Linyan, Li Qingfang, Wang Yexiao, Zhang Yiwen, Ma Xuelei
State Key Laboratory of Biotherapy and Cancer Center, West China Hospital, Sichuan University and Collaborative Innovation Center, Chengdu, PR China.
Oncotarget. 2017 Aug 9;8(45):79854-79863. doi: 10.18632/oncotarget.20078. eCollection 2017 Oct 3.
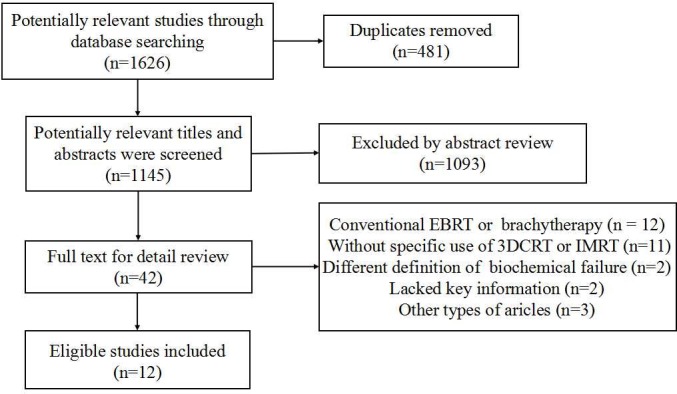
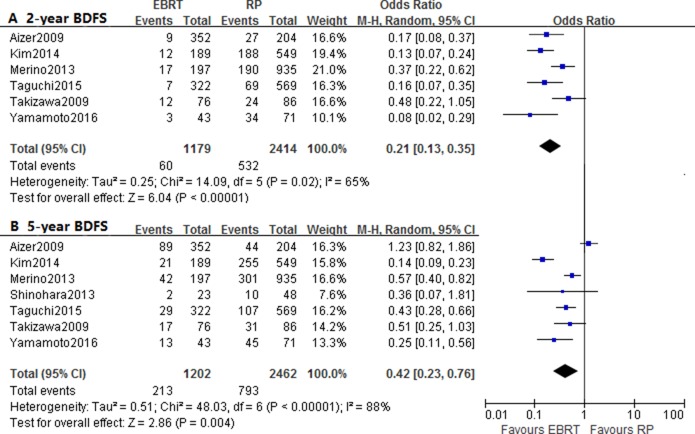
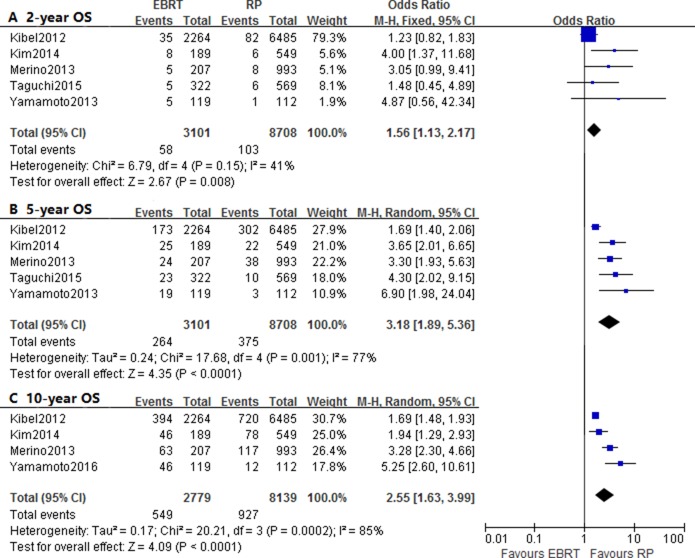
Since there was no consensus on treatment options of localized prostate cancer, a meta-analysis was performed to compare the efficacy of radical prostatectomy (RP) versus external beam radiotherapy (EBRT) concluding three-dimensional conformal radiotherapy (3DCRT) and intensity-modulated radiation therapy (IMRT). The search of eligible studies was performed on PubMed and Embase databases. The overall survival (OS), cancer-specific survival (CSS) and biochemical disease-free survival (BDFS) were compared by hazard ratio (HR) and odd ratios (OR). Twelve studies with 17137 patients were included. The pooled HR and 95% CI for OS, CSS and BDFS were 1.60 (1.44-1.79), 1.73 (1.34-2.24) and 0.65 (0.51-0.82), respectively. However, according to risk stratification, the HRs of CSS for low- to intermediate-risk patients were not significant. The 5-year and 10-year CSS reported significant OR and 95% CI of 1.96 (1.42-2.72) and 2.44 (1.33-4.48), except for 2-year CSS ( 0.42). In conclusion, RP was generally associated with decreased risk of overall and cancer-specific mortality as well as better 5-year and 10-year OS and CSS. The EBRT was suggested to be a promising alternative option for low- to intermediate-risk patients. Large-scale prospective studies with risk stratification and adequate follow-up length were needed for further comprehensive comparison.
由于局部前列腺癌的治疗方案尚无共识,因此进行了一项荟萃分析,以比较根治性前列腺切除术(RP)与外照射放疗(EBRT,包括三维适形放疗(3DCRT)和调强放疗(IMRT))的疗效。在PubMed和Embase数据库中检索符合条件的研究。通过风险比(HR)和比值比(OR)比较总生存期(OS)、癌症特异性生存期(CSS)和生化无病生存期(BDFS)。纳入了12项研究,共17137例患者。OS、CSS和BDFS的合并HR及95%置信区间分别为1.60(1.44 - 1.79)、1.73(1.34 - 2.24)和0.65(0.51 - 0.82)。然而,根据风险分层,低至中危患者CSS的HR无统计学意义(此处原文有误,根据前文逻辑推测,应是低至中危患者CSS的HR无显著差异)。除2年CSS(0.42)外,5年和10年CSS的OR及95%置信区间分别为1.96(1.42 - 2.72)和2.44(1.33 - 4.48)。总之,RP通常与总体和癌症特异性死亡风险降低以及更好的5年和10年OS及CSS相关。对于低至中危患者,EBRT被认为是一种有前景的替代选择。需要进行大规模的前瞻性研究,进行风险分层并保证足够的随访时间,以进行进一步全面比较。