Division of Radiation Oncology, Aizawa Comprehensive Cancer Center, Aizawa Hospital, 2-5-1, Honjo, Matsumoto-city, Nagano-prefecturem, Japan.
Positron Imaging Center, Aizawa Hospital, 2-5-1, Honjo, Matsumoto-city, Nagano-prefecturem, Japan.
BMC Cancer. 2017 Nov 6;17(1):713. doi: 10.1186/s12885-017-3702-x.
On conventional diagnostic imaging, the features of radiation necrosis (RN) are similar to those of local recurrence (LR) of brain metastases (BM). C-methionine positron emission tomography (MET-PET) is reportedly useful for making a differential diagnosis between LR and RN. In this prospective study, we aimed to investigate the diagnostic performance of MET-PET and the long-term results of subsequent patient management.
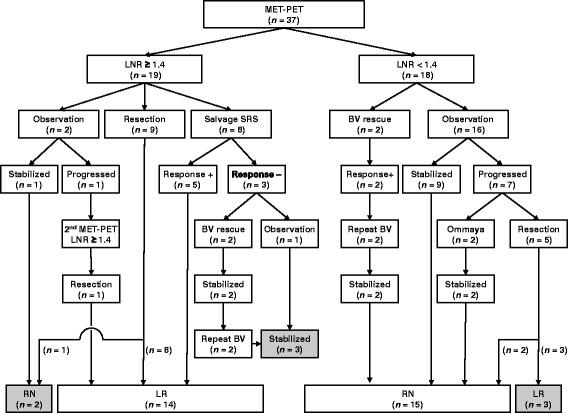
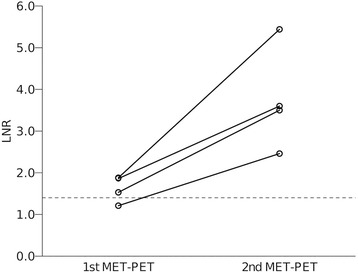
The eligible subjects had enlarging contrast-enhanced lesions (>1 cm) on MR imaging after any form of radiotherapy for BM, suggesting LR or RN. However, it was difficult to differentiate LR from RN in these cases. From August 2013 to February 2017, MET-PET was performed for 37 lesions in 32 eligible patients. Tracer accumulation in the regions of interest was analysed as the standardised uptake value (SUV) and maximal lesion SUV/maximal normal tissue SUV ratios (LNR) were calculated. The cut-off value for LNR was provisionally set at 1.40. Salvage treatment strategies determined based on MET-PET diagnosis and treatment results were investigated. The diagnostic accuracy of MET-PET was evaluated by receiver operating characteristic (ROC) curve analysis.
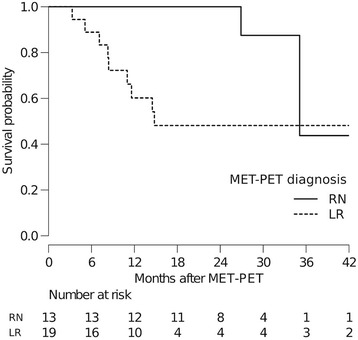
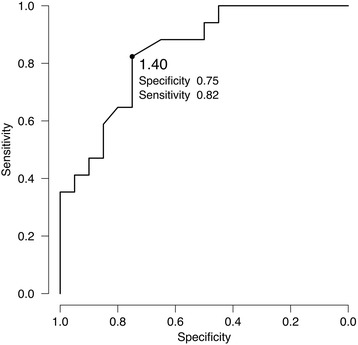
The median interval from primary radiotherapy to MET-PET was 19 months and radiotherapy had been performed twice or more for 13 lesions. The MET-PET diagnoses were LR in 19 and RN in 18 lesions. The mean values and standard deviation of LNRs for each diagnostic category were 1.70 ± 0.30 and 1.09 ± 0.25, respectively. At the median follow-up time of 18 months, final diagnoses were confirmed histologically for 17 lesions and clinically for 20 lesions. ROC curve analysis indicated the optimal LNR cut-off value to be 1.40 (area under the curve: 0.84), and the sensitivity and specificity were 0.82 and 0.75, respectively. The median survival times of patient groups with LR and RN based on MET-PET diagnosis were 14.8 months and 35.1 months, respectively (P = 0.035, log-rank test).
MET-PET showed apparently reliable diagnostic performance for distinguishing between LR and RN. The provisional LNR cut-off value of 1.4 in our institution was found to be appropriate. Limitations of diagnostic accuracy should be recognised in cases with LNR close to this cut-off value.
在常规诊断影像学中,放射性坏死 (RN) 的特征与脑转移瘤 (BM) 的局部复发 (LR) 相似。据报道,C-蛋氨酸正电子发射断层扫描 (MET-PET) 可用于鉴别 LR 和 RN。在这项前瞻性研究中,我们旨在研究 MET-PET 的诊断性能以及后续患者管理的长期结果。
符合条件的患者在接受任何形式的 BM 放疗后,MR 成像上出现增大的对比增强病变(>1cm),提示 LR 或 RN。然而,在这些情况下,LR 与 RN 很难区分。从 2013 年 8 月至 2017 年 2 月,对 32 名符合条件的患者的 37 个病灶进行了 MET-PET 检查。分析感兴趣区域的示踪剂积聚作为标准化摄取值 (SUV),并计算最大病变 SUV/最大正常组织 SUV 比值 (LNR)。暂定 LNR 的截断值设定为 1.40。根据 MET-PET 诊断和治疗结果确定的挽救治疗策略进行了调查。通过受试者工作特征 (ROC) 曲线分析评估 MET-PET 的诊断准确性。
从原发放疗到 MET-PET 的中位时间间隔为 19 个月,13 个病灶接受了两次或两次以上放疗。MET-PET 诊断为 LR 的有 19 个病灶,RN 的有 18 个病灶。每个诊断类别的 LNR 平均值和标准差分别为 1.70±0.30 和 1.09±0.25。在 18 个月的中位随访时间内,17 个病灶的最终诊断得到了组织学证实,20 个病灶得到了临床证实。ROC 曲线分析表明,最佳 LNR 截断值为 1.40(曲线下面积:0.84),灵敏度和特异性分别为 0.82 和 0.75。根据 MET-PET 诊断,LR 和 RN 患者组的中位生存时间分别为 14.8 个月和 35.1 个月(P=0.035,对数秩检验)。
MET-PET 对鉴别 LR 和 RN 具有明显可靠的诊断性能。我们机构的暂定 LNR 截断值为 1.4 似乎是合适的。在接近该截断值的 LNR 病例中,应认识到诊断准确性的局限性。