Department of HIV, World Health Organization, Geneva, Switzerland.
Centre for Infectious Disease Epidemiology and Research, University of Cape Town, Cape Town, South Africa.
AIDS. 2018 Jan 2;32(1):17-23. doi: 10.1097/QAD.0000000000001671.
Recent attention has focused on the question of how quickly antiretroviral therapy (ART) should be started once HIV diagnosis is confirmed. We assessed whether rapid ART initiation improves patient outcomes.
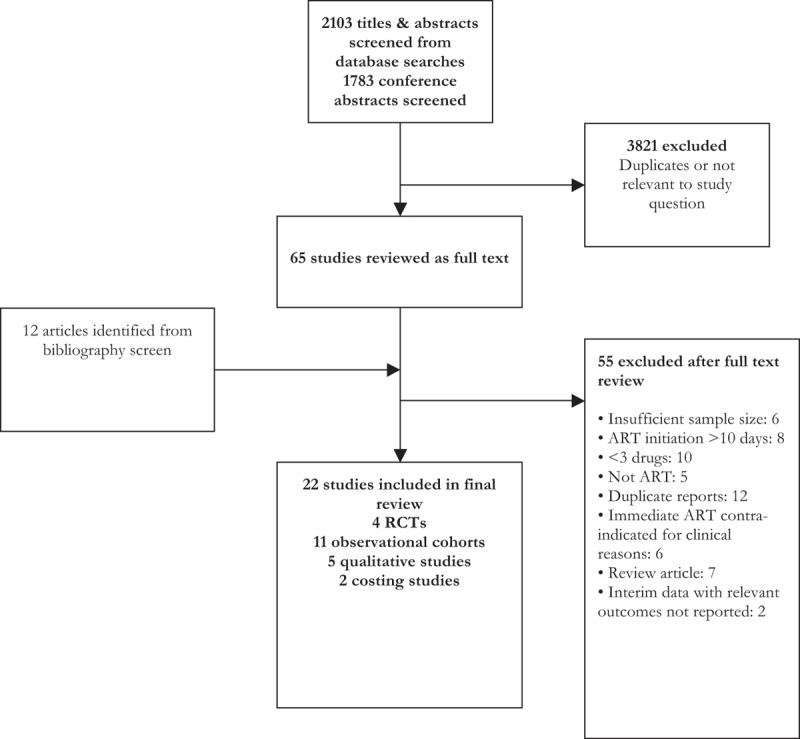
We searched five databases from inception up to August 2017. Rapid ART initiation was defined as initiation within 14 days of HIV diagnosis. Data were pooled using random effects meta-analysis.
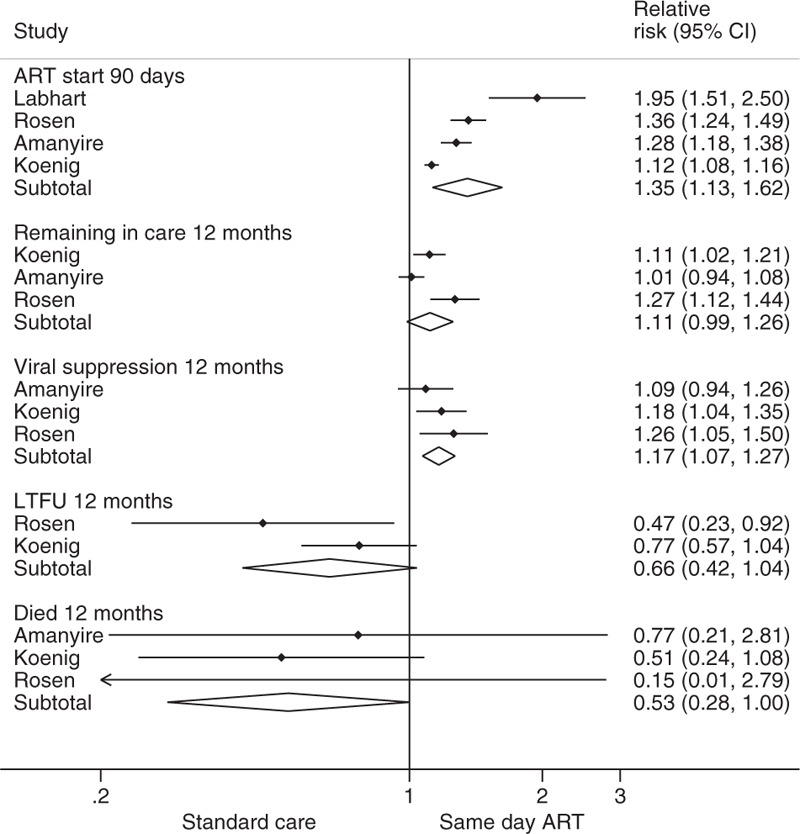
Across the randomized trials, ART start on the same day increased viral suppression at 12 months [three trials: relative risk (RR) 1.17, 95% confidence interval (CI) 1.07-1.27], retention in care at 12 months (RR 1.11, 95% CI 0.99-1.26), and the likelihood of starting ART within 90 days (four trials: RR 1.35, 95% CI 1.13-1.62) and 12 months after eligibility was established (three trials: RR 1.17, 95% CI 1.07-1.27). There was a nonsignificant trend toward reduced mortality (three trials: RR 0.53, 95% CI 0.24-1.08), as well as reduced loss to follow-up at 12 months (2 trials: RR 0.66, 95% CI 0.42-1.04). In the observational studies, offering accelerated ART initiation resulted in a greater likelihood of having started ART within 3 months (two studies: RR 1.53, 95% CI 1.11-2.10). There was a trend toward an increased risk of being lost to follow-up at 6 months (three studies: RR 1.85, 95% CI 0.96-3.55).
Accelerated ART initiation can lead to improved clinical outcomes and is likely to be of particular benefit in those settings where extensive patient preparation prior to starting ART results in long delays. These findings informed a WHO recommendation supporting accelerated ART initiation, including same day ART start.
最近人们关注的焦点是一旦确诊 HIV 后,应多快开始抗逆转录病毒治疗(ART)。我们评估了快速开始 ART 是否能改善患者结局。
我们从建库起至 2017 年 8 月检索了 5 个数据库。快速开始 ART 定义为在 HIV 诊断后 14 天内开始。采用随机效应荟萃分析汇总数据。
在随机试验中,同日开始 ART 可提高 12 个月时的病毒抑制率[3 项试验:相对风险(RR)1.17,95%置信区间(CI)1.07-1.27]、12 个月时的保留在治疗中率(RR 1.11,95%CI 0.99-1.26)以及在符合条件后 90 天(4 项试验:RR 1.35,95%CI 1.13-1.62)和 12 个月(3 项试验:RR 1.17,95%CI 1.07-1.27)内开始 ART 的可能性。死亡率有降低的趋势(3 项试验:RR 0.53,95%CI 0.24-1.08),12 个月时失访率也有降低的趋势(2 项试验:RR 0.66,95%CI 0.42-1.04)。在观察性研究中,加速 ART 开始使 3 个月内开始 ART 的可能性增加(2 项研究:RR 1.53,95%CI 1.11-2.10)。6 个月时失访的风险有增加的趋势(3 项研究:RR 1.85,95%CI 0.96-3.55)。
加速 ART 开始可改善临床结局,在开始 ART 前需要进行广泛患者准备导致长时间延迟的情况下,可能尤其有益。这些发现为世卫组织支持加速 ART 开始的建议提供了信息,包括同日开始 ART。