Elimova Elena, Slack Rebecca S, Chen Hsiang-Chun, Planjery Venkatram, Shiozaki Hironori, Shimodaira Yusuke, Charalampakis Nick, Lin Quan, Harada Kazuto, Wadhwa Roopma, Estrella Jeannelyn S, Kaya Dilsa Mizrak, Sagebiel Tara, Lee Jeffrey H, Weston Brian, Bhutani Manoop, Murphy Mariela Blum, Matamoros Aurelio, Minsky Bruce, Das Prajnan, Mansfield Paul F, Badgwell Brian D, Ajani Jaffer A
Department of Gastrointestinal Medical Oncology, The University of Texas M.D. Anderson Cancer Center, Houston, TX, USA.
Department of Medical Oncology, Princess Margaret Cancer Centre, University of Toronto, Toronto, ON, Canada.
Oncotarget. 2017 Jul 13;8(46):81430-81440. doi: 10.18632/oncotarget.19226. eCollection 2017 Oct 6.
After therapy of localized gastric adenocarcinoma (GAC) patients, the costs of surveillance, relapse patterns, and possibility of salvage are unknown.
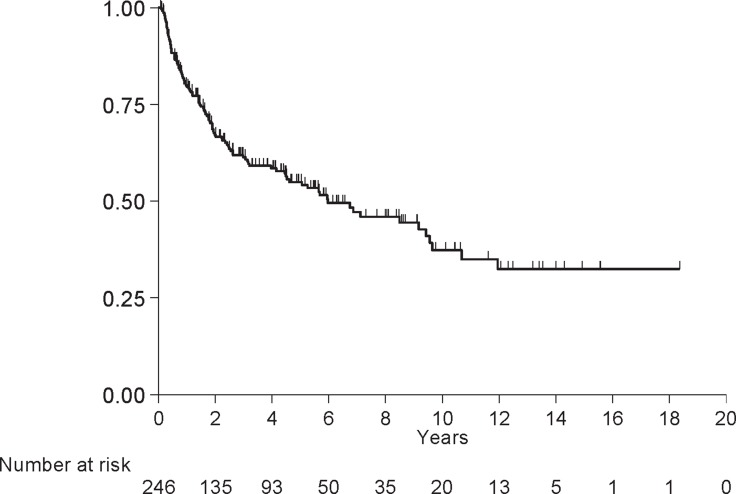
We identified 246 patients, who after having a negative peritoneal staging, received therapy (any therapy which included surgery) and were surveyed (every 3-6 months in the first 3 years, then yearly; ∼10 CTs and ∼7 endoscopies per patient). We used the 2016 Medicare dollars reimbursed as the "costs" for surveillance.
Common features were: Caucasians (57%), men (60%), poorly differentiated histology (76%), preoperative chemotherapy (74%), preoperative chemoradiation (59%), and had surgery (100%). At a median follow-up of 3.7 years (range, 0.1 to 18.3), the median overall survival (OS) was 9.2 years (95% CI, 6.0 to 11.2). Tumor grade ( = 0.02), p/yp stage ( < 0.001), % residual GAC ( = 0.05), the R status ( = 0.01), total gastrectomy ( = 0.001), and relapse type ( = 0.02) were associated with OS. Relapse occurred in 79 (32%) patients (only 8% were local-regional) and 90% occurred within 36 months of surgery. P/yp stage ( < 0.001) and total gastrectomy ( = 0.01) were independent prognosticators for OS in the multivariate analysis. Only 1 relapsed patient had successful salvage therapy. The estimated reimbursement for imaging studies and endoscopies was $1,761,221.91 (marked underestimation of actual costs).
The median OS of localized GAC patients was excellent with infrequent local-regional relapses. Rigorous surveillance had a low yield and high "costs". Our data suggest that less frequent surveillance intervals and limiting expensive investigations to symptomatic patients may be warranted.
局部性胃腺癌(GAC)患者接受治疗后,监测成本、复发模式及挽救的可能性尚不清楚。
我们确定了246例患者,这些患者在腹膜分期为阴性后接受了治疗(包括手术的任何治疗)并接受了随访(前3年每3 - 6个月一次,之后每年一次;每位患者约10次CT和7次内镜检查)。我们将2016年医疗保险报销金额用作监测“成本”。
常见特征为:白种人(57%)、男性(60%)、组织学分化差(76%)、术前化疗(74%)、术前放化疗(59%)且均接受了手术(100%)。中位随访时间为3.7年(范围0.1至18.3年),中位总生存期(OS)为9.2年(95%CI,6.0至11.2)。肿瘤分级( = 0.02)、p/yp分期( < 0.001)、残余GAC百分比( = 0.05)、R状态( = 0.01)、全胃切除术( = 0.001)及复发类型( = 0.02)与总生存期相关。79例(32%)患者出现复发(仅8%为局部区域复发),90%的复发发生在手术后36个月内。在多变量分析中,p/yp分期( < 0.001)和全胃切除术( = 0.01)是总生存期独立的预后因素。仅有1例复发患者接受了成功的挽救治疗。影像学检查和内镜检查的估计报销费用为1,761,221.91美元(实际成本被严重低估)。
局部性GAC患者的中位总生存期良好,局部区域复发不常见。严格的监测收益低且“成本”高。我们的数据表明,可能有必要减少监测间隔频率,并将昂贵的检查限制在有症状的患者中。