Department of Urology, Institute of Nephrourology, Victoria Hospital Campus, Bangalore, India.
Investig Clin Urol. 2017 Nov;58(6):453-459. doi: 10.4111/icu.2017.58.6.453. Epub 2017 Oct 27.
Urosepsis implies clinically evident severe infection of urinary tract with features of systemic inflammatory response syndrome (SIRS). We validate the role of a single Acute Physiology and Chronic Health Evaluation II (APACHE II) score at 24 hours after admission in predicting mortality in urosepsis.
A prospective observational study was done in 178 patients admitted with urosepsis in the Department of Urology, in a tertiary care institute from January 2015 to August 2016. Patients >18 years diagnosed as urosepsis using SIRS criteria with positive urine or blood culture for bacteria were included. At 24 hours after admission to intensive care unit, APACHE II score was calculated using 12 physiological variables, age and chronic health.
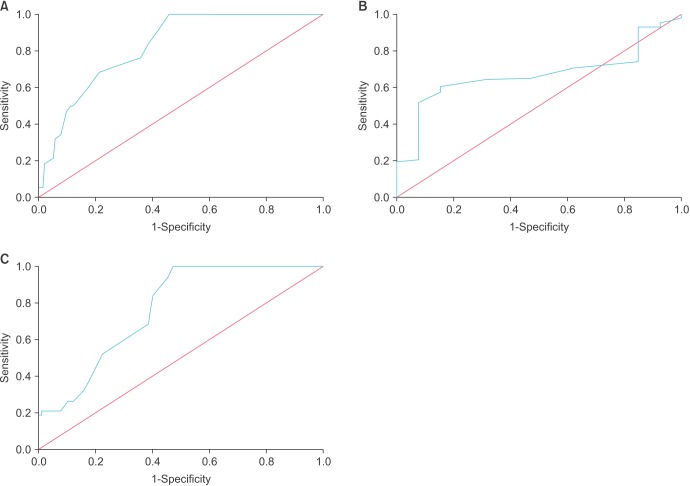
Mean±standard deviation (SD) APACHE II score was 26.03±7.03. It was 24.31±6.48 in survivors and 32.39±5.09 in those expired (p<0.001). Among patients undergoing surgery, mean±SD score was higher (30.74±4.85) than among survivors (24.30±6.54) (p<0.001). Receiver operating characteristic (ROC) analysis revealed area under curve (AUC) of 0.825 with cutoff 25.5 being 94.7% sensitive and 56.4% specific to predict mortality. Mean±SD score in those undergoing surgery was 25.22±6.70 and was lesser than those who did not undergo surgery (28.44±7.49) (p=0.007). ROC analysis revealed AUC of 0.760 with cutoff 25.5 being 94.7% sensitive and 45.6% specific to predict mortality even after surgery.
A single APACHE II score assessed at 24 hours after admission was able to predict morbidity, mortality, need for surgical intervention, length of hospitalization, treatment success and outcome in urosepsis patients.
尿脓毒症是指尿路感染伴有全身炎症反应综合征(SIRS)的临床明显严重感染。我们验证了入院 24 小时后单个急性生理学和慢性健康评估 II(APACHE II)评分在预测尿脓毒症患者死亡率中的作用。
这是一项前瞻性观察研究,在 2015 年 1 月至 2016 年 8 月期间,在一家三级护理机构的泌尿科,对 178 名患有尿脓毒症的患者进行了该研究。纳入标准为:使用 SIRS 标准诊断为尿脓毒症,尿液或血液培养细菌阳性的>18 岁患者。在入住重症监护病房 24 小时后,使用 12 个生理变量、年龄和慢性健康状况计算 APACHE II 评分。
平均±标准差(SD)APACHE II 评分为 26.03±7.03。存活者为 24.31±6.48,死亡者为 32.39±5.09(p<0.001)。接受手术的患者的平均±SD 评分(30.74±4.85)高于存活者(24.30±6.54)(p<0.001)。接受手术的患者的受试者工作特征(ROC)分析显示,曲线下面积(AUC)为 0.825,截断值为 25.5,其预测死亡率的敏感性为 94.7%,特异性为 56.4%。接受手术的患者的平均±SD 评分为 25.22±6.70,低于未接受手术的患者(28.44±7.49)(p=0.007)。ROC 分析显示,截断值为 25.5,其预测死亡率的敏感性为 94.7%,特异性为 45.6%,即使在手术后也有一定效果。
入院 24 小时后评估的单个 APACHE II 评分能够预测尿脓毒症患者的发病率、死亡率、手术干预需求、住院时间、治疗成功率和预后。