Department of Radiology, University of Groningen, University Medical Center Groningen, the Netherlands; Athinoula A. Martinos Center for Biomedical Imaging, Department of Radiology, Massachusetts General Hospital and Harvard-MIT Health Science and Technology, USA.
Department of Nuclear Medicine and Molecular Imaging, University of Groningen, University Medical Center Groningen, the Netherlands; Department of Biomedical Photonic Imaging, University of Twente, the Netherlands.
J Magn Reson Imaging. 2018 Apr;47(4):891-912. doi: 10.1002/jmri.25885. Epub 2017 Nov 13.
Although cardiac MR and T mapping are increasingly used to diagnose diffuse fibrosis based cardiac diseases, studies reporting T values in healthy and diseased myocardium, particular in nonischemic cardiomyopathies (NICM) and populations with increased cardiovascular risk, seem contradictory.
To determine the range of native myocardial T value ranges in patients with NICM and populations with increased cardiovascular risk.
Systemic review and meta-analysis.
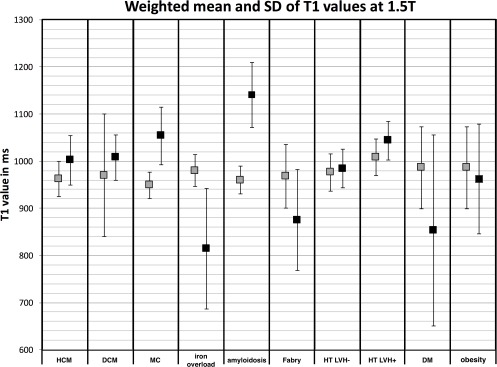
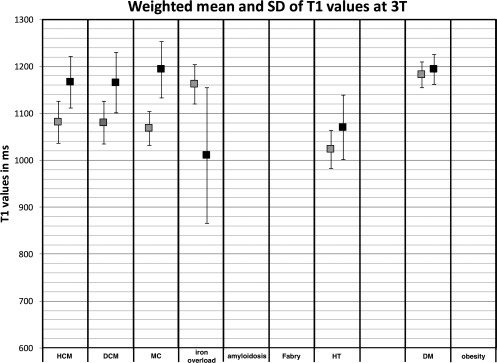
Patients with NICM, including hypertrophic cardiomyopathy (HCM) and dilated cardiomyopathy (DCM), and patients with myocarditis (MC), iron overload, amyloidosis, Fabry disease, and populations with hypertension (HT), diabetes mellitus (DM), and obesity. FIELD STRENGTH/SEQUENCE: (Shortened) modified Look-Locker inversion-recovery MR sequence at 1.5 or 3T.
PubMed and Embase were searched following the PRISMA guidelines.
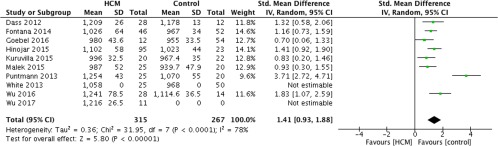
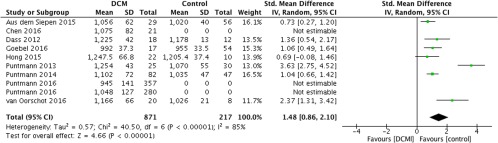
The summary of standard mean difference (SMD) between the diseased and a healthy control populations was generated using a random-effects model in combination with meta-regression analysis.
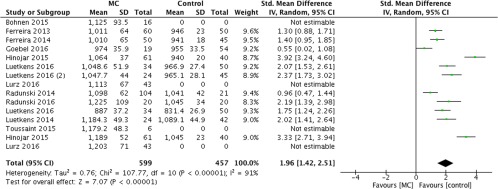
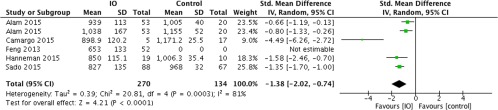
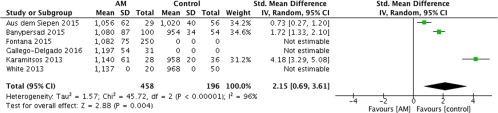
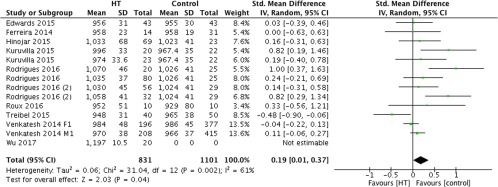
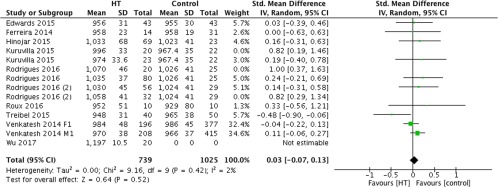
The SMD for HCM, DCM, and MC patients were significantly increased (1.41, 1.48, and 1.96, respectively, P < 0.01) compared with healthy controls. The SMD for HT patients with and without left-ventricle hypertrophy (LVH) together was significantly increased (0.19, P = 0.04), while for HT patients without LVH the SMD was zero (0.03, P = 0.52). The number of studies on amyloidosis, iron overload, Fabry disease, and HT patients with LVH did not meet the requirement to perform a meta-analysis. However, most studies reported a significantly increased T for amyloidosis and HT patients with LVH and a significant decreased T for iron overload and Fabry disease patients.
Native T mapping by using an (Sh)MOLLI sequence can potentially assess myocardial changes in HCM, DCM, MC, iron overload, amyloidosis, and Fabry disease compared to controls. In addition, it can help to diagnose left-ventricular remodeling in HT patients.
2 Technical Efficacy: Stage 3 J. Magn. Reson. Imaging 2018;47:891-912.
尽管心脏磁共振和 T 映射技术越来越多地用于诊断弥漫性纤维化性心脏病,但报告健康和患病心肌 T 值的研究结果似乎存在矛盾,特别是在非缺血性心肌病(NICM)和心血管风险增加的人群中。
确定 NICM 患者和心血管风险增加人群的心肌固有 T 值范围。
系统评价和荟萃分析。
NICM 患者,包括肥厚型心肌病(HCM)和扩张型心肌病(DCM)以及心肌炎(MC)、铁过载、淀粉样变性、Fabry 病患者,以及高血压(HT)、糖尿病(DM)和肥胖患者。场强/序列:(缩短的)改良 Look-Locker 反转恢复 MR 序列,场强为 1.5 或 3T。
根据 PRISMA 指南对 PubMed 和 Embase 进行了搜索。
采用随机效应模型结合荟萃回归分析,生成患病人群与健康对照组之间标准均数差(SMD)的汇总。
与健康对照组相比,HCM、DCM 和 MC 患者的 SMD 显著增加(分别为 1.41、1.48 和 1.96,P<0.01)。HT 患者伴或不伴左心室肥厚(LVH)的 SMD 均显著增加(0.19,P=0.04),而 HT 患者无 LVH 的 SMD 为零(0.03,P=0.52)。淀粉样变性、铁过载、Fabry 病和 HT 患者伴 LVH 的研究数量未达到进行荟萃分析的要求。然而,大多数研究报告称,淀粉样变性和 HT 患者伴 LVH 的 T 值显著增加,而铁过载和 Fabry 病患者的 T 值显著降低。
使用(Sh)MOLLI 序列进行心肌固有 T 映射可用于评估 HCM、DCM、MC、铁过载、淀粉样变性和 Fabry 病与对照组相比心肌的变化。此外,它可以帮助诊断 HT 患者的左心室重构。
2 技术功效:第 3 阶段 J. Magn. Reson. Imaging 2018;47:891-912.