Grunau Gilat L, Gueron Shay, Pornov Boris, Linn Shai
Department of Radiology, University of British Columbia, Vancouver, British Columbia, Canada.
Department of Mathematics, University of Haifa, Haifa, Israel.
Rambam Maimonides Med J. 2018 Jan 29;9(1):e0002. doi: 10.5041/RMMJ.10321.
Estimates of lifetime cancer risk are commonly used in the clinical setting and in health-care evaluations. These measures are based on lifetime cancer risk estimates and may create an unrealistically frightening perception of cancer risk for an individual. We suggest using two new measures of cancer risk to complement the cancer lifetime risk measure, namely estimates of cancer risk from birth to a specific age or from a specific age to life expectancy.
We calculated risks using incidence density data from the Israel National Cancer Registry of 2013, applying a well-known formula for calculating risk, for a follow-up time. The joint disease-free survival probability is calculated for several age intervals, and hence the risk (i.e. 1-survival) for the intervals.
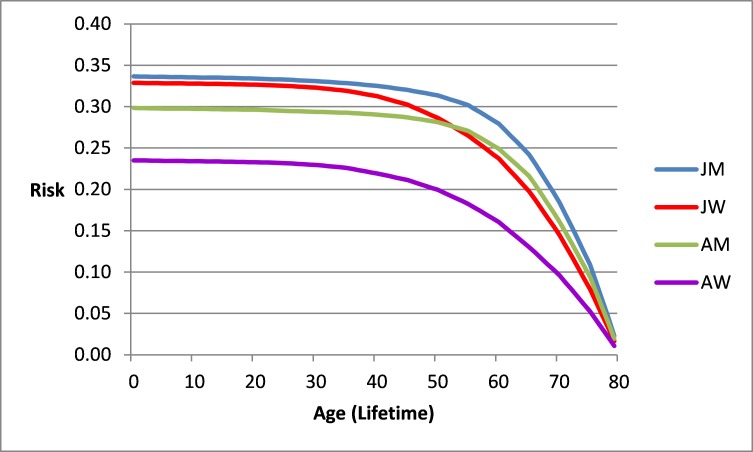
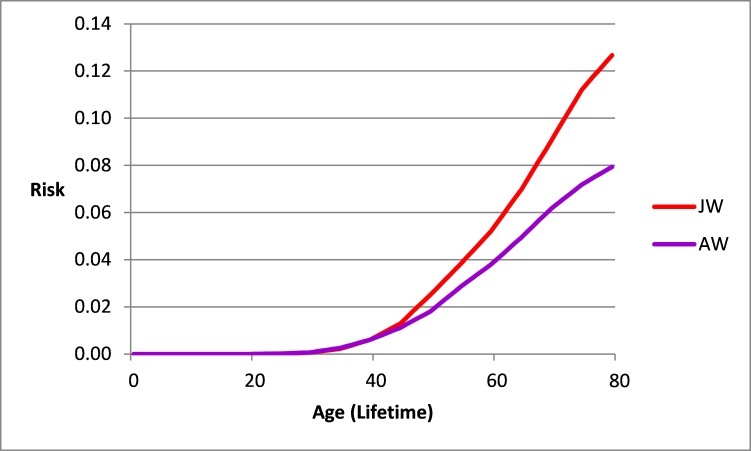
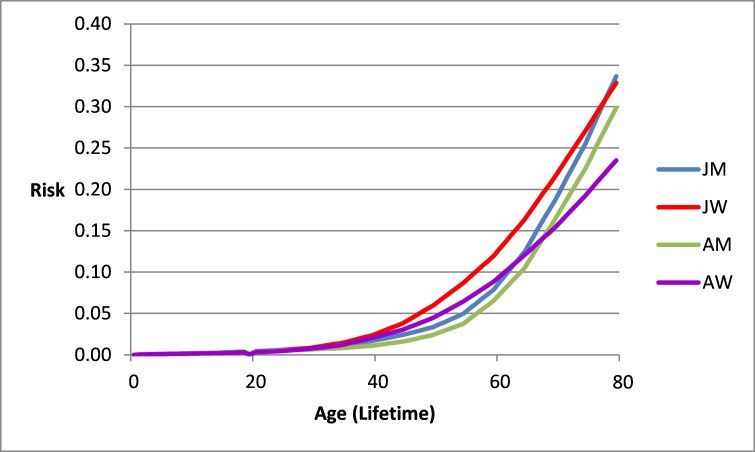
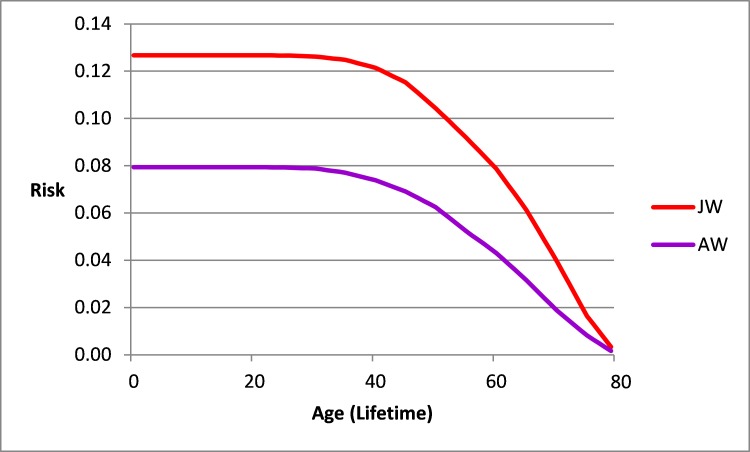
The risk of cancer to age 80 in Jewish men and women, respectively, ranged from about 0.336 and 0.329 at age 0, to 0.279 and 0.237 at age 60. The risk of cancer from birth up to an age in Jewish men and women, respectively, ranged from 0 and 0 at birth to 0.088 and 0.129 at age 60. The risk of cancer to age 80 in Arab men and women, respectively, ranged from 0.298 and 0.235 at age 0 to 0.249 and 0.161 at age 60. The risk of cancer from birth up to an age in Arab men and women, respectively, ranged from 0 and 0 at age 0 to 0.074 and 0.095 at age 60. In Jewish and Arab women, breast cancer risk to age 80 decreased from about 0.127 in Jewish women at age 40 to 0.079 at age 60 and from 0.080 to 0.043 in Arab women; the risk from birth up to a specific age ranged between 0 and 0.056, and 0 and 0.040, respectively.
The two proposed new estimates convey important additional information to patients and physicians. These estimates are considerably lower than the frequently quoted 33% lifetime cancer risk and are more relevant to patients and physicians. Similarly, breast cancer risk estimates up to or from a specific age differ considerably from the frequently quoted lifetime risk estimates of 1 in 8 women.
终生癌症风险估计值常用于临床环境和医疗保健评估中。这些测量基于终生癌症风险估计,可能会给个体造成对癌症风险不切实际的恐惧认知。我们建议使用两种新的癌症风险测量方法来补充癌症终生风险测量方法,即从出生到特定年龄或从特定年龄到预期寿命的癌症风险估计。
我们使用2013年以色列国家癌症登记处的发病密度数据计算风险,应用一个著名的风险计算公式,并设定随访时间。计算几个年龄区间的联合无病生存概率,进而得出这些区间的风险(即1减去生存概率)。
犹太男性和女性到80岁时的癌症风险,分别从0岁时的约0.336和0.329,降至60岁时的0.279和0.237。犹太男性和女性从出生到某一年龄的癌症风险,分别从出生时的0和0,增至60岁时的0.088和0.129。阿拉伯男性和女性到80岁时的癌症风险,分别从0岁时的0.298和0.235,降至60岁时的0.249和0.161。阿拉伯男性和女性从出生到某一年龄的癌症风险,分别从0岁时的0和0,增至60岁时的0.074和0.095。在犹太和阿拉伯女性中,到80岁时的乳腺癌风险从犹太女性40岁时的约0.127降至60岁时的0.079,在阿拉伯女性中从0.080降至0.043;从出生到特定年龄的风险分别在0至0.056和0至0.040之间。
这两种新提出的估计值能向患者和医生传达重要的额外信息。这些估计值远低于经常引用的33%终生癌症风险,对患者和医生而言更具相关性。同样,特定年龄之前或到特定年龄的乳腺癌风险估计值与经常引用的八分之一女性终生风险估计值有很大差异。