From the Department of Neurology (Neurocritical Care) (N.H., R.A.C., M.W.K., R.C., W.H., S.M.), Department of Psychiatry (N.H.), Department of Surgery (R.C., W.H., S.M.), and Department of Anesthesia/Critical Care (R.C., S.M.), University of Massachusetts Medical School, Worcester, Massachusetts.
J Trauma Acute Care Surg. 2018 Mar;84(3):473-482. doi: 10.1097/TA.0000000000001733.
Diffuse axonal injury (DAI) on magnetic resonance imaging has been associated with poor functional outcome after moderate-severe traumatic brain injury (msTBI). Yet, DAI assessment with highly sensitive magnetic resonance imaging techniques is unfeasible in the acute trauma setting, and computed tomography (CT) remains the key diagnostic modality despite its lower sensitivity. We sought to determine whether CT-defined hemorrhagic DAI (hDAI) is associated with discharge and favorable 3- and 12-month functional outcome (Glasgow Coma Scale score ≥4) after msTBI.
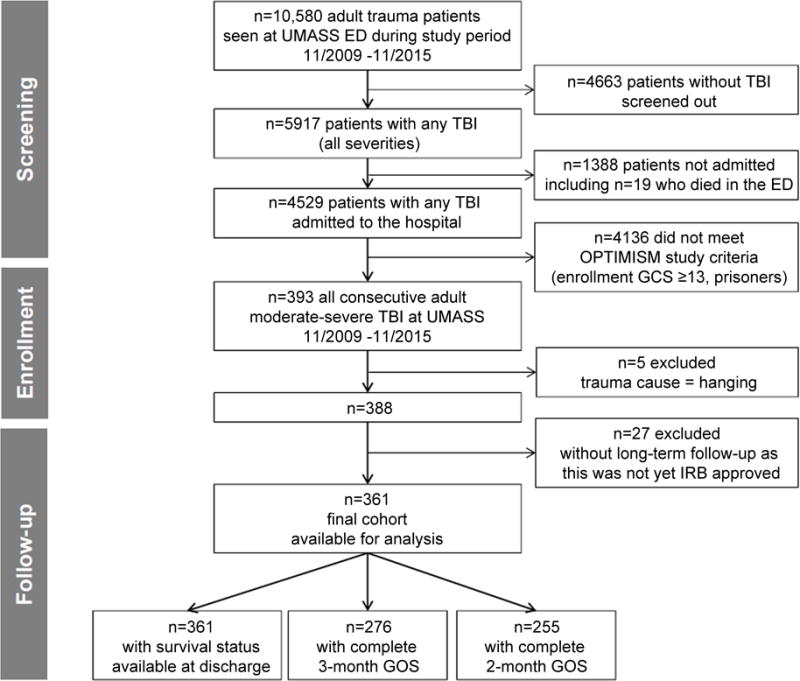
We analyzed 361 msTBI patients from the single-center longitudinal Outcome Prognostication in Traumatic Brain Injury study collected over 6 years (November 2009 to November 2015) with prospective outcome assessments at 3 months and 12 months. Patients with microhemorrhages on CT were designated "CT-hDAI-positive" and those without as "CT-hDAI-negative." For secondary analyses "CT-hDAI-positive" was stratified into two phenotypes according to presence ("associated") versus absence ("predominant") of concomitant large acute traumatic lesions to determine whether presence versus absence of additional focal mass lesions portends a different prognosis.
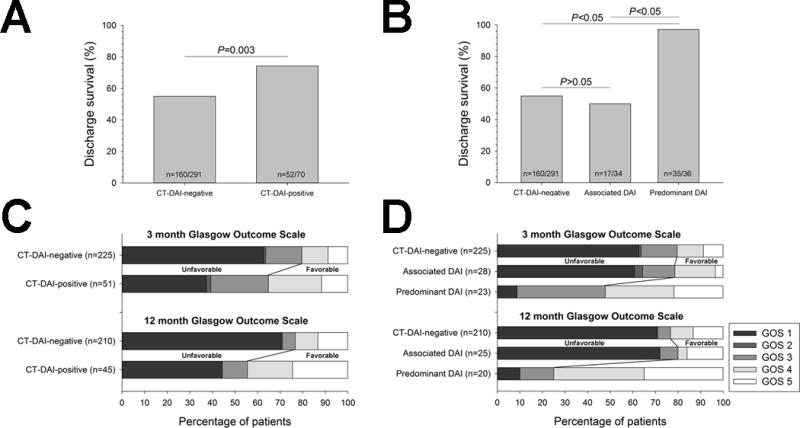
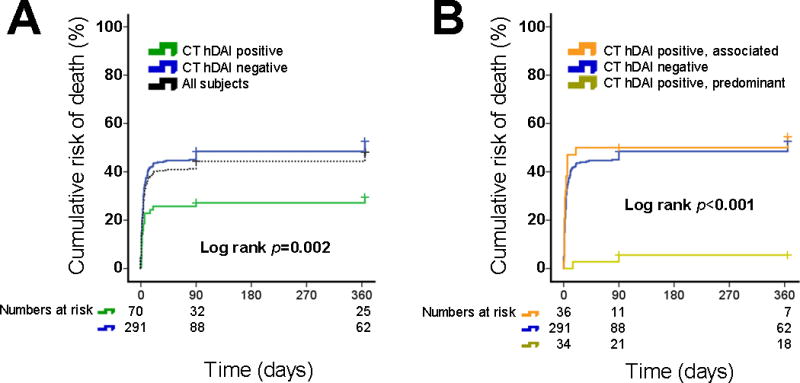
Seventy (19%) patients were CT-hDAI-positive (n = 36 predominant; n = 34 associated hDAI). In univariate analyses, CT-hDAI-positive status was associated with discharge survival (p = 0.004) and favorable outcome at 3 months (p = 0.003) and 12 months (p = 0.005). After multivariable adjustment, CT-hDAI positivity was no longer associated with discharge survival and functional outcome (all ps > 0.05). Stratified by hDAI phenotype, predominant hDAI patients had worse trauma severity, longer intensive care unit stays, and more systemic medical complications. Predominant hDAI, but not associated hDAI, was an independent predictor of discharge survival (adjusted odds ratio, 24.7; 95% confidence interval [CI], 3.2-192.6; p = 0.002) and favorable 12-month outcome (adjusted odds ratio, 4.7; 95% CI, 1.5-15.2; p = 0.01). Sensitivity analyses using Cox regression confirmed this finding for 1-year survival (adjusted hazard ratio, 5.6; 95% CI, 1.3-23; p = 0.048).
The CT-defined hDAI was not an independent predictor of unfavorable short- and long-term outcomes and should not be used for acute prognostication in msTBI patients. Predominant hDAI patients had good clinical outcomes when supported to intensive care unit discharge and beyond.
Prognostic study, level III.
磁共振成像上的弥漫性轴索损伤(DAI)与中重度创伤性脑损伤(msTBI)后的功能预后不良相关。然而,在急性创伤环境下使用高度敏感的磁共振成像技术评估 DAI 是不可行的,而计算机断层扫描(CT)仍然是关键的诊断方式,尽管其敏感性较低。我们旨在确定 CT 定义的出血性 DAI(hDAI)是否与 msTBI 后的出院和 3 个月和 12 个月的有利功能结局(格拉斯哥昏迷量表评分≥4)相关。
我们分析了来自单中心纵向创伤性脑损伤预后研究的 361 例 msTBI 患者,该研究在 6 年内(2009 年 11 月至 2015 年 11 月)进行了前瞻性结局评估,3 个月和 12 个月时进行了随访。CT 上有微出血的患者被指定为“CT-hDAI 阳性”,无微出血的患者为“CT-hDAI 阴性”。为了进行二次分析,根据是否存在(“相关”)或不存在(“主要”)同时存在的大急性创伤性病变,将“CT-hDAI 阳性”分为两种表型,以确定是否存在或不存在额外的局灶性肿块病变预示着不同的预后。
70 例(19%)患者为 CT-hDAI 阳性(n=36 例主要表现;n=34 例相关 hDAI)。在单变量分析中,CT-hDAI 阳性状态与出院生存率(p=0.004)和 3 个月(p=0.003)和 12 个月(p=0.005)的良好结局相关。多变量调整后,CT-hDAI 阳性与出院生存率和功能结局均不再相关(均 p>0.05)。按 hDAI 表型分层,主要 hDAI 患者的创伤严重程度更高、重症监护病房停留时间更长且合并更多的全身医学并发症。主要的 hDAI 而不是相关的 hDAI 是出院生存率的独立预测因素(调整后的优势比,24.7;95%置信区间[CI],3.2-192.6;p=0.002)和 12 个月时的良好结局(调整后的优势比,4.7;95%CI,1.5-15.2;p=0.01)。使用 Cox 回归的敏感性分析证实了这一发现,即 1 年生存率(调整后的危险比,5.6;95%CI,1.3-23;p=0.048)。
CT 定义的 hDAI 不是不利的短期和长期结局的独立预测因素,不应用于 msTBI 患者的急性预后评估。在支持患者转出重症监护病房并进行后续治疗时,主要的 hDAI 患者有良好的临床结局。
预后研究,III 级。