Lee Ji Ye, Park Ji Eun, Shim Woo Hyun, Jung Seung Chai, Choi Choong Gon, Kim Sang Joon, Kim Jeong Hoon, Kim Ho Sung
Department of Radiology, Soonchunhyang University Bucheon Hospital, 170 Jomaru-ro, Wonmi-gu, Bucheon, Korea.
Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea.
PLoS One. 2017 Nov 15;12(11):e0187989. doi: 10.1371/journal.pone.0187989. eCollection 2017.
Distinguishing non-neoplastic pituitary stalk lesions (non-NPSLs) from neoplastic pituitary stalk lesions (NPSLs) is a major concern in guiding treatment for a thickened pituitary stalk. Our study aimed to aid provide preoperative diagnostic assistance by combining clinical and magnetic resonance imaging (MRI) findings to distinguish non-NPSLs from NPSLs.
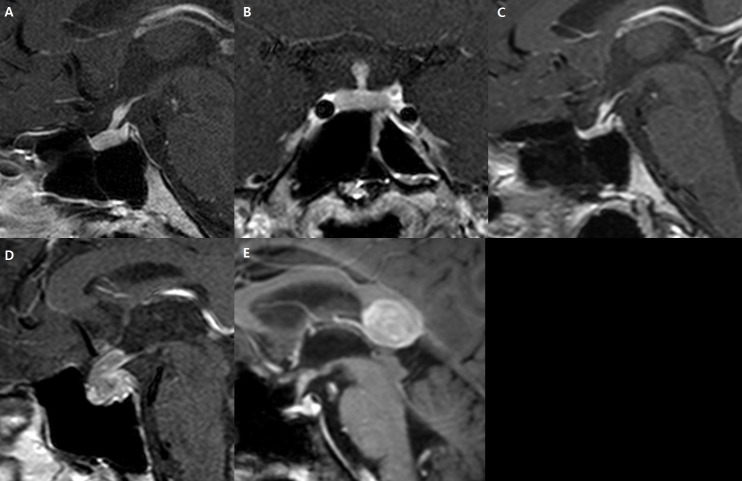
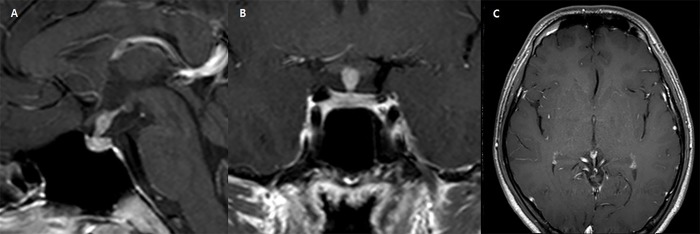
We recruited 158 patients with thickened pituitary stalk lesions visible on MRI. Laboratory findings included hypopituitarism, diabetes insipidus (DI), and hyperprolactinemia. MR images were assessed for anterior-posterior thickness (mm), diffuse pituitary stalk thickening, cystic changes, a high T1 signal, and glandular or extrasellar involvement. A diagnostic model was developed using a recursive partitioning logistic regression analysis. The model was validated in an independent dataset comprising 63 patients, and its diagnostic performance was compared with that of the original radiological reports.
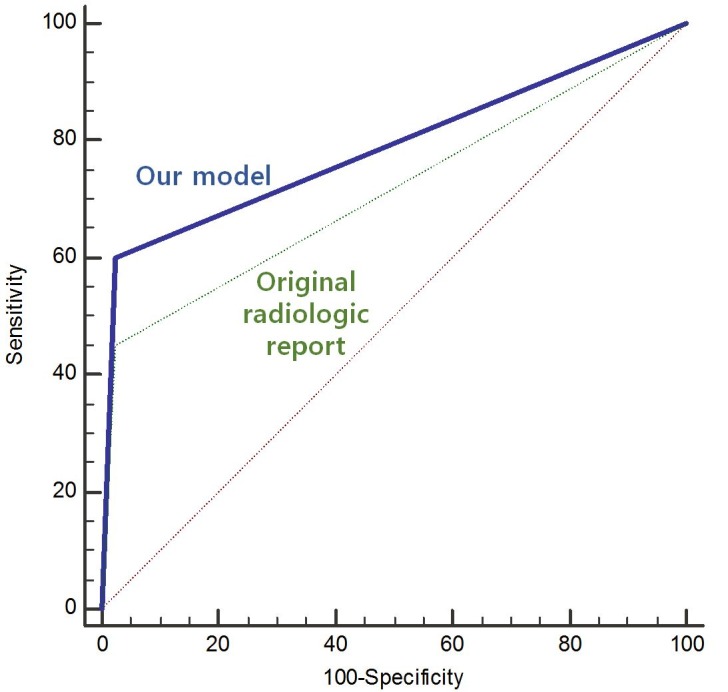
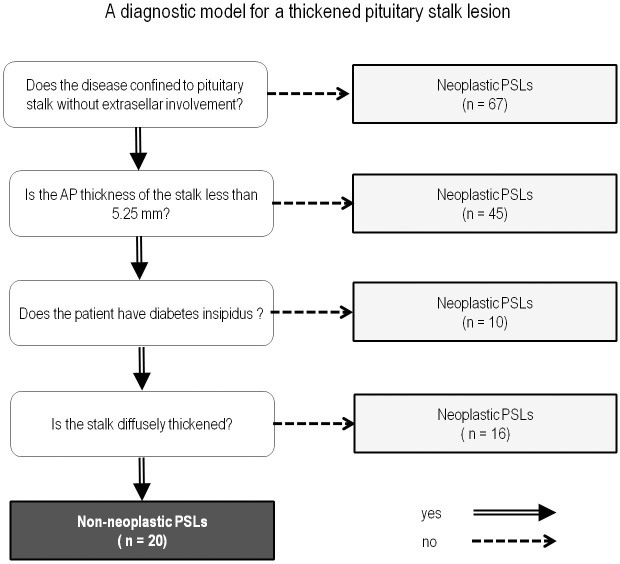
A univariate analysis found significant associations of DI (P = 0.006), absence of extrasellar involvement (P = 0.002), and lower stalk thickness (P = 0.031) with non-NPSLs. A diagnostic model was created using the following parameters (in order of priority): 1) lack of extrasellar involvement, 2) stalk thickness < 5.3 mm, and 3) presence of DI. The diagnostic performance (area under the curve; AUC) of this model in the independent set was 0.813, representing a significant improvement over the original radiological reports (AUC: 0.713, P = 0.029).
The joint diagnostic approach based on clinical and imaging-based factors robustly distinguished non-NPSLs from NPSLs. This approach could guide treatment strategies and prevent unnecessary surgery in patients with non-NPSL.
区分非肿瘤性垂体柄病变(non-NPSLs)与肿瘤性垂体柄病变(NPSLs)是指导垂体柄增粗治疗的主要关注点。我们的研究旨在通过结合临床和磁共振成像(MRI)结果来区分non-NPSLs与NPSLs,以提供术前诊断帮助。
我们招募了158例MRI可见垂体柄增粗病变的患者。实验室检查结果包括垂体功能减退、尿崩症(DI)和高催乳素血症。对MR图像评估前后径厚度(mm)、垂体柄弥漫性增粗、囊性改变、T1高信号以及腺体内或鞍外受累情况。使用递归划分逻辑回归分析建立诊断模型。该模型在包含63例患者的独立数据集中进行验证,并将其诊断性能与原始放射学报告的诊断性能进行比较。
单因素分析发现DI(P = 0.006)、无鞍外受累(P = 0.002)和较低的垂体柄厚度(P = 0.031)与non-NPSLs显著相关。使用以下参数(按优先级顺序)创建诊断模型:1)无鞍外受累,2)垂体柄厚度<5.3 mm,3)存在DI。该模型在独立数据集中的诊断性能(曲线下面积;AUC)为0.813,相较于原始放射学报告(AUC:0.713,P = 0.029)有显著改善。
基于临床和影像学因素的联合诊断方法能有力地区分non-NPSLs与NPSLs。这种方法可指导治疗策略,并防止non-NPSL患者进行不必要的手术。