Bello Aminu K, Qarni Bilal, Samimi Arian, Okel Julius, Chatterley Trish, Okpechi Ikechi G, Vandermeer Ben, Braam Branko
Division of Nephrology and Immunology, Department of Medicine, University of Alberta, Edmonton, Canada.
John W. Scott Health Sciences Library, University of Alberta, Edmonton, Canada.
Kidney Int Rep. 2017 Feb 16;2(4):617-625. doi: 10.1016/j.ekir.2017.02.007. eCollection 2017 Jul.
The risk of major adverse events associated with chronic kidney disease (CKD) could potentially be reduced with effective medical interventions. The impact of multifaceted interventions as compared with usual care in patients with nondiabetic CKD is unclear. We performed a systematic review to analyze the impact of multifaceted interventions on reducing the risk of major adverse events in this population.
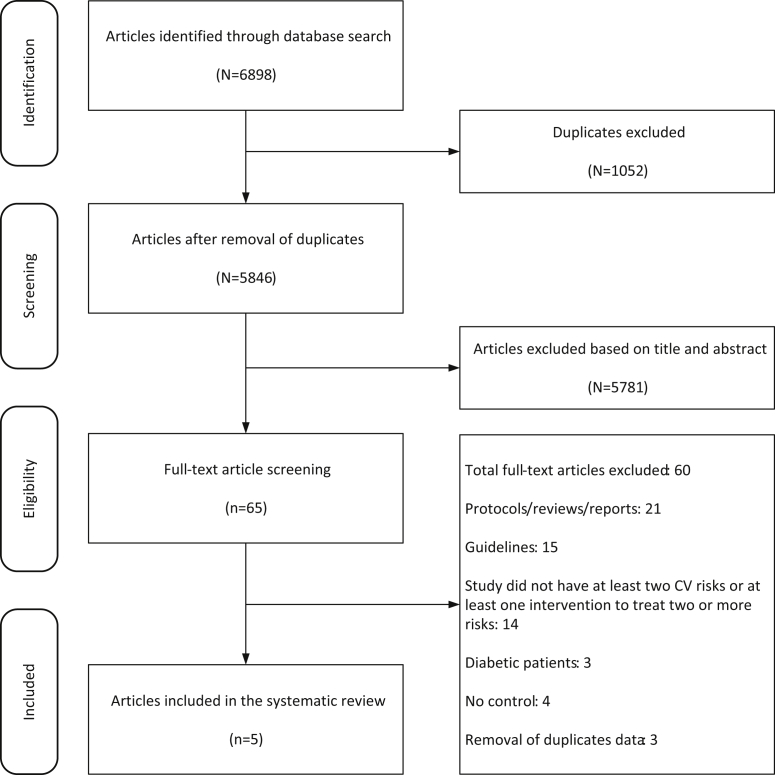
Systematic review and meta-analysis. We searched MEDLINE, EMBASE, CINAHL and the Cochrane Library databases for medical literature published up to November 2016. Published original studies and abstracts were reviewed that reported on adult patients in a community or specialty care setting, with 2 or more CKD risk factors, treated with a combination of more than 2 interventions. We included randomized controlled trials, observational studies, and systematic reviews. Studies focused on diabetic patients were excluded. The intervention was defined as a treatment with a combination of 2 or more interventions compared with the usual care. The outcomes were defined as a reduction in the risk of adverse clinical outcomes (renal replacement therapy, all-cause hospitalizations, all-cause and cardiovascular mortality, cardiovascular events) as primary outcomes. Secondary outcomes were optimal risk factor control (attaining guideline concordant blood pressure, reduction of proteinuria, smoking cessation).
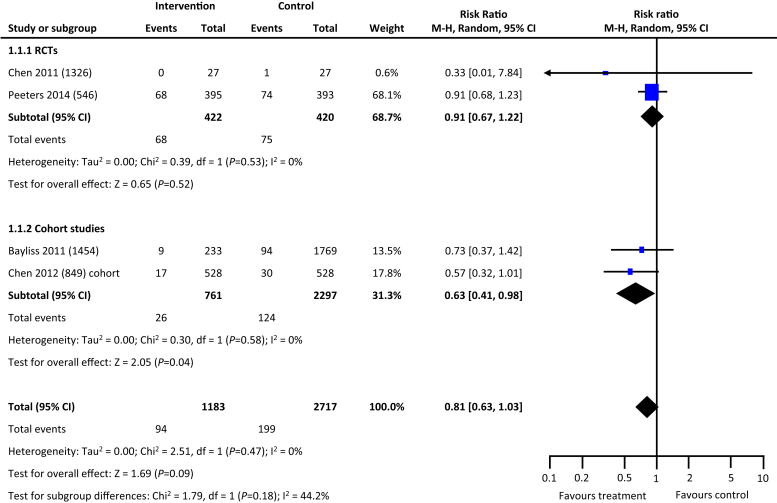
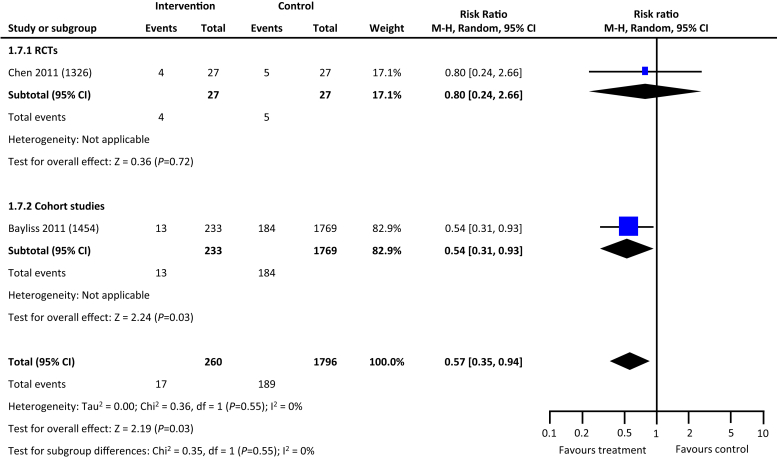
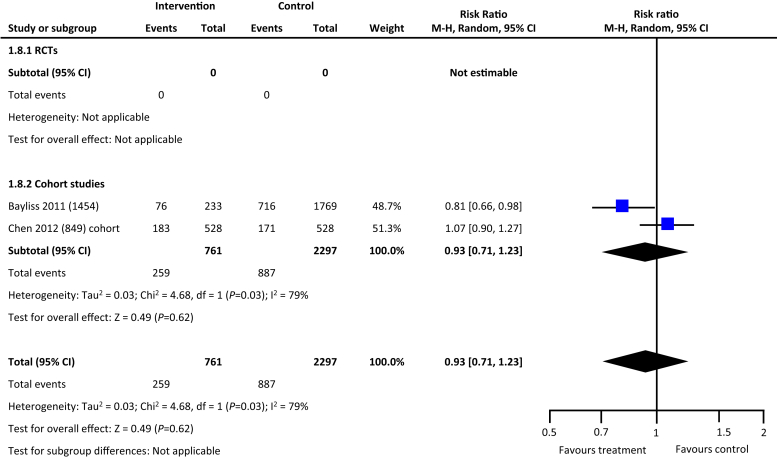
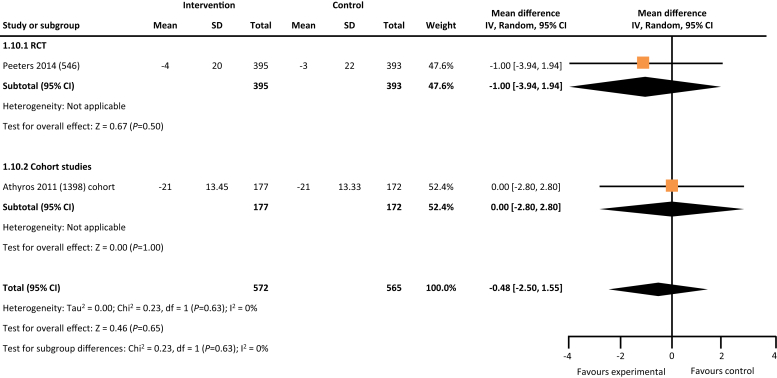
Five of the 5846 unique citations from our initial literature search met our study criteria. All identified studies reported on patients with CKD and their management. In comparison with usual care, multifaceted interventions tended to reduce all-cause mortality (risk ratio: 0.81, 95% confidence interval: 0.63-1.03) and were associated with a lower risk of progression to kidney failure requiring dialysis (risk ratio: 0.57, 95% confidence interval: 0.35-0.94). Multifaceted interventions were not associated with reducing risk of all-cause hospitalizations (risk ratio: 0.93, 95% confidence interval: 0.71-1.23) or improved blood pressure control (mean difference: -0.48, range: -2.5 to 1.55 mm Hg).
Multifaceted interventions targeting multiple risk factors tended to reduce the risk of all-cause mortality and reduced the risk to progress to end-stage kidney failure in patients with CKD. There is a need for high-quality studies that can rigorously evaluate a set of interventions targeting multiple domains of CKD management in the population with nondiabetic CKD due to paucity of data in the current published literature.
有效的医学干预措施有可能降低与慢性肾脏病(CKD)相关的重大不良事件风险。与常规治疗相比,多方面干预措施对非糖尿病CKD患者的影响尚不清楚。我们进行了一项系统评价,以分析多方面干预措施对降低该人群重大不良事件风险的影响。
系统评价和荟萃分析。我们检索了MEDLINE、EMBASE、CINAHL和Cochrane图书馆数据库,以获取截至2016年11月发表的医学文献。对已发表的原始研究和摘要进行了综述,这些研究报告了社区或专科护理环境中的成年患者,有2个或更多CKD危险因素,接受了2种以上干预措施的联合治疗。我们纳入了随机对照试验、观察性研究和系统评价。聚焦糖尿病患者的研究被排除。干预措施定义为2种或更多干预措施联合治疗与常规治疗的比较。结局定义为不良临床结局(肾脏替代治疗、全因住院、全因和心血管死亡率、心血管事件)风险降低作为主要结局。次要结局为最佳危险因素控制(达到指南一致的血压、降低蛋白尿、戒烟)。
我们初步文献检索得到的5846条独特引用文献中有5条符合我们的研究标准。所有纳入研究均报告了CKD患者及其管理情况。与常规治疗相比,多方面干预措施倾向于降低全因死亡率(风险比:0.81,95%置信区间:0.63-1.03),并与进展至需要透析的肾衰竭风险较低相关(风险比:0.57,95%置信区间:0.35-0.94)。多方面干预措施与降低全因住院风险(风险比:0.93,95%置信区间:0.71-1.23)或改善血压控制(平均差值:-0.48,范围:-2.5至1.55 mmHg)无关。
针对多种危险因素的多方面干预措施倾向于降低全因死亡率,并降低CKD患者进展至终末期肾衰竭的风险。由于当前已发表文献中的数据匮乏,需要高质量的研究来严格评估针对非糖尿病CKD人群CKD管理多个领域的一组干预措施。