Tangri Navdeep, Grams Morgan E, Levey Andrew S, Coresh Josef, Appel Lawrence J, Astor Brad C, Chodick Gabriel, Collins Allan J, Djurdjev Ognjenka, Elley C Raina, Evans Marie, Garg Amit X, Hallan Stein I, Inker Lesley A, Ito Sadayoshi, Jee Sun Ha, Kovesdy Csaba P, Kronenberg Florian, Heerspink Hiddo J Lambers, Marks Angharad, Nadkarni Girish N, Navaneethan Sankar D, Nelson Robert G, Titze Stephanie, Sarnak Mark J, Stengel Benedicte, Woodward Mark, Iseki Kunitoshi
Department of Medicine, Seven Oaks General Hospital, University of Manitoba, Winnipeg, Canada2Department of Community Health Sciences, Seven Oaks General Hospital, University of Manitoba, Winnipeg, Canada.
Johns Hopkins Medical Institutions, Baltimore, Maryland.
JAMA. 2016 Jan 12;315(2):164-74. doi: 10.1001/jama.2015.18202.
Identifying patients at risk of chronic kidney disease (CKD) progression may facilitate more optimal nephrology care. Kidney failure risk equations, including such factors as age, sex, estimated glomerular filtration rate, and calcium and phosphate concentrations, were previously developed and validated in 2 Canadian cohorts. Validation in other regions and in CKD populations not under the care of a nephrologist is needed.
To evaluate the accuracy of the risk equations across different geographic regions and patient populations through individual participant data meta-analysis.
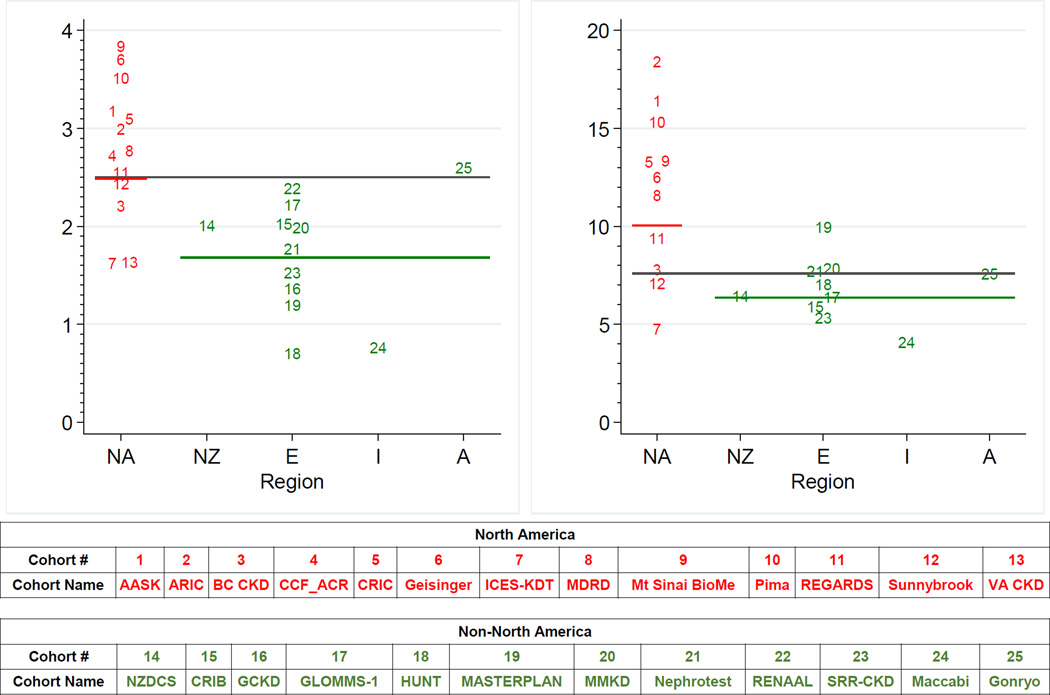
Thirty-one cohorts, including 721,357 participants with CKD stages 3 to 5 in more than 30 countries spanning 4 continents, were studied. These cohorts collected data from 1982 through 2014.
Cohorts participating in the CKD Prognosis Consortium with data on end-stage renal disease.
Data were obtained and statistical analyses were performed between July 2012 and June 2015. Using the risk factors from the original risk equations, cohort-specific hazard ratios were estimated and combined using random-effects meta-analysis to form new pooled kidney failure risk equations. Original and pooled kidney failure risk equation performance was compared, and the need for regional calibration factors was assessed.
Kidney failure (treatment by dialysis or kidney transplant).
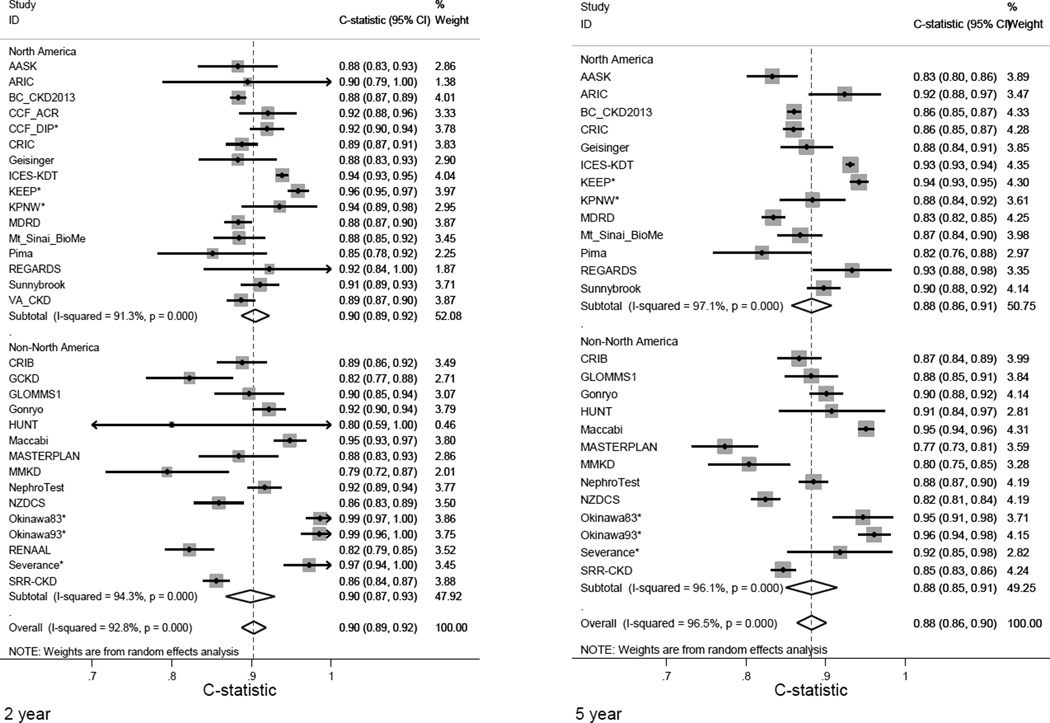
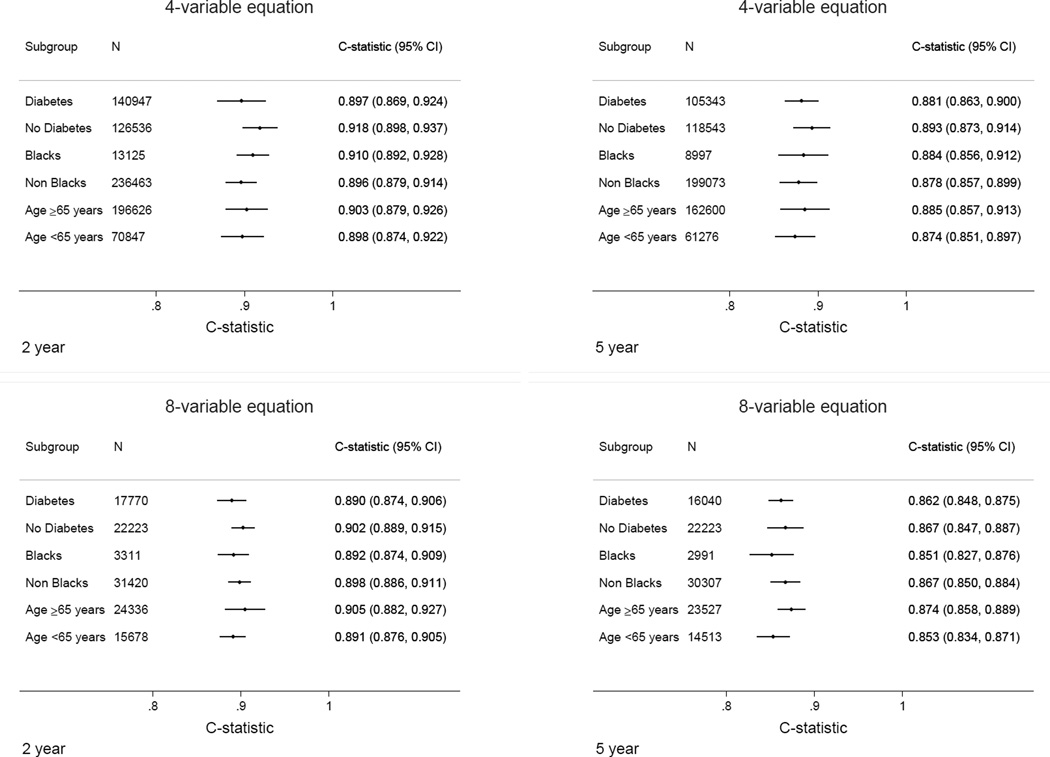
During a median follow-up of 4 years of 721,357 participants with CKD, 23,829 cases kidney failure were observed. The original risk equations achieved excellent discrimination (ability to differentiate those who developed kidney failure from those who did not) across all cohorts (overall C statistic, 0.90; 95% CI, 0.89-0.92 at 2 years; C statistic at 5 years, 0.88; 95% CI, 0.86-0.90); discrimination in subgroups by age, race, and diabetes status was similar. There was no improvement with the pooled equations. Calibration (the difference between observed and predicted risk) was adequate in North American cohorts, but the original risk equations overestimated risk in some non-North American cohorts. Addition of a calibration factor that lowered the baseline risk by 32.9% at 2 years and 16.5% at 5 years improved the calibration in 12 of 15 and 10 of 13 non-North American cohorts at 2 and 5 years, respectively (P = .04 and P = .02).
Kidney failure risk equations developed in a Canadian population showed high discrimination and adequate calibration when validated in 31 multinational cohorts. However, in some regions the addition of a calibration factor may be necessary.
识别有慢性肾脏病(CKD)进展风险的患者可能有助于提供更优化的肾脏病护理。此前已开发出肾衰竭风险方程,纳入了年龄、性别、估计肾小球滤过率以及钙和磷浓度等因素,并在2个加拿大队列中进行了验证。还需要在其他地区以及未接受肾脏病专科医生治疗的CKD人群中进行验证。
通过个体参与者数据荟萃分析评估风险方程在不同地理区域和患者人群中的准确性。
对31个队列进行了研究,这些队列包括来自四大洲30多个国家的721357例CKD 3至5期患者。这些队列收集了1982年至2014年的数据。
参与CKD预后联盟且有终末期肾病数据的队列。
于2012年7月至2015年6月获取数据并进行统计分析。利用原始风险方程中的风险因素,估计队列特异性风险比,并采用随机效应荟萃分析进行合并,以形成新的汇总肾衰竭风险方程。比较原始和汇总的肾衰竭风险方程的性能,并评估是否需要区域校准因子。
肾衰竭(透析或肾移植治疗)。
在721357例CKD参与者的中位随访4年期间,观察到23829例肾衰竭病例。原始风险方程在所有队列中均表现出出色的区分度(区分发生肾衰竭者与未发生者的能力)(总体C统计量为0.90;2年时95%CI为0.89 - 0.92;5年时C统计量为0.88;95%CI为0.86 - 0.90);按年龄、种族和糖尿病状态分组的亚组中的区分度相似。汇总方程并无改善。北美队列的校准(观察到的风险与预测风险之间的差异)是合适的,但原始风险方程在一些非北美队列中高估了风险。添加一个校准因子,在2年时将基线风险降低32.9%,在5年时降低16.5%,分别改善了15个非北美队列中12个队列在2年时以及13个非北美队列中10个队列在5年时的校准(P = 0.04和P = 0.02)。
在加拿大人群中开发的肾衰竭风险方程在31个跨国队列中验证时显示出高区分度和合适的校准。然而,在某些地区可能需要添加校准因子。