de Boer Dolf, van der Hoek Lucas, Rademakers Jany, Delnoij Diana, van den Berg Michael
Netherlands Institute for Health Services Research, Otterstraat 118-124, 3513CR, Utrecht, The Netherlands.
Department of Family Medicine, CAPHRI (School for Public Health and Primary Care), Maastricht University, Maastricht, The Netherlands.
BMC Health Serv Res. 2017 Nov 22;17(1):768. doi: 10.1186/s12913-017-2732-z.
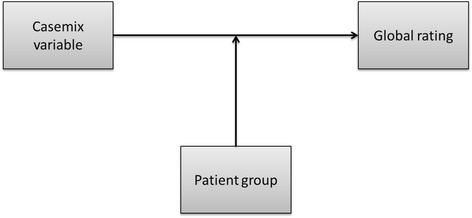
Many survey studies in health care adjust for demographic characteristics such as age, gender, educational attainment and general health when performing statistical analyses. Whether the effects of these demographic characteristics are consistent between patient groups remains to be determined. This is important as the rationale for adjustment is often that demographic sub-groups differ in their so-called 'response tendency'. This rationale may be less convincing if the effects of response tendencies vary across patient groups. The present paper examines whether the impact of these characteristics on patients' global rating of care varies across patient groups.
Secondary analyses using multi-level regression models were performed on a dataset including 32 different patient groups and 145,578 observations. For each demographic variable, the 95% expected range of case-mix coefficients across patient groups is presented. In addition, we report whether the variance of coefficients for demographic variables across patient groups is significant.
Overall, men, elderly, lower educated people and people in good health tend to give higher global ratings. However, these effects varied significantly across patient groups and included the possibility of no effect or an opposite effect in some patient groups.
The response tendency attributed to demographic characteristics - such as older respondents being milder, or higher educated respondents being more critical - is not general or universal. As such, the mechanism linking demographic characteristics to survey results on patient experiences with quality of care is more complicated than a general response tendency. It is possible that the response tendency interacts with patient group, but it is also possible that other mechanisms are at play.
许多医疗保健领域的调查研究在进行统计分析时会对年龄、性别、教育程度和总体健康状况等人口统计学特征进行调整。这些人口统计学特征的影响在不同患者群体之间是否一致仍有待确定。这一点很重要,因为调整的理由通常是人口统计学亚组在其所谓的“反应倾向”上存在差异。如果反应倾向的影响在不同患者群体中有所不同,那么这个理由可能就不那么有说服力了。本文研究了这些特征对患者总体护理评分的影响在不同患者群体中是否存在差异。
对一个包含32个不同患者群体和145578条观察数据的数据集进行了二级分析,使用多层次回归模型。对于每个人口统计学变量,给出了不同患者群体中病例组合系数的95%预期范围。此外,我们报告了不同患者群体中人口统计学变量系数的方差是否显著。
总体而言,男性、老年人、受教育程度较低者和健康状况良好者往往给出较高的总体评分。然而,这些影响在不同患者群体中差异显著,包括在某些患者群体中可能没有影响或有相反影响的情况。
归因于人口统计学特征的反应倾向——比如年龄较大的受访者更温和,或受教育程度较高的受访者更挑剔——并非普遍存在。因此,将人口统计学特征与患者护理质量体验调查结果联系起来的机制比一般的反应倾向更为复杂。反应倾向有可能与患者群体相互作用,但也有可能是其他机制在起作用。