Mayo Clinic, Rochester, MN, USA.
Memorial Sloan Kettering Cancer Center, New York, NY, USA.
Haematologica. 2018 Feb;103(2):297-303. doi: 10.3324/haematol.2017.176511. Epub 2017 Nov 23.
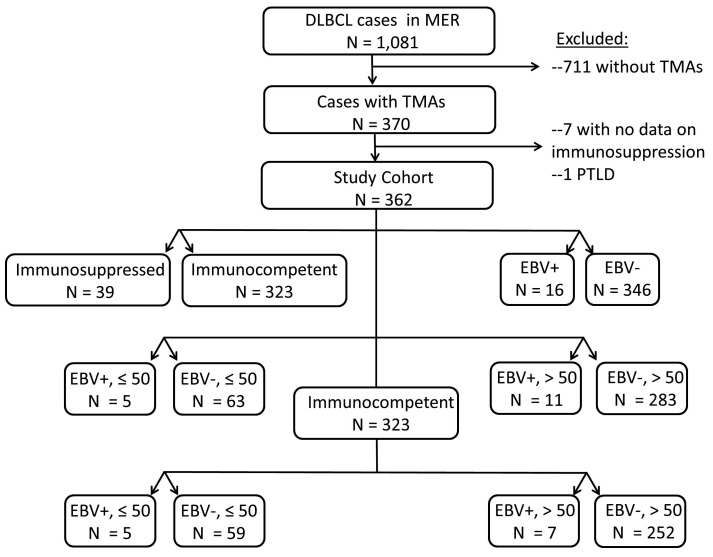
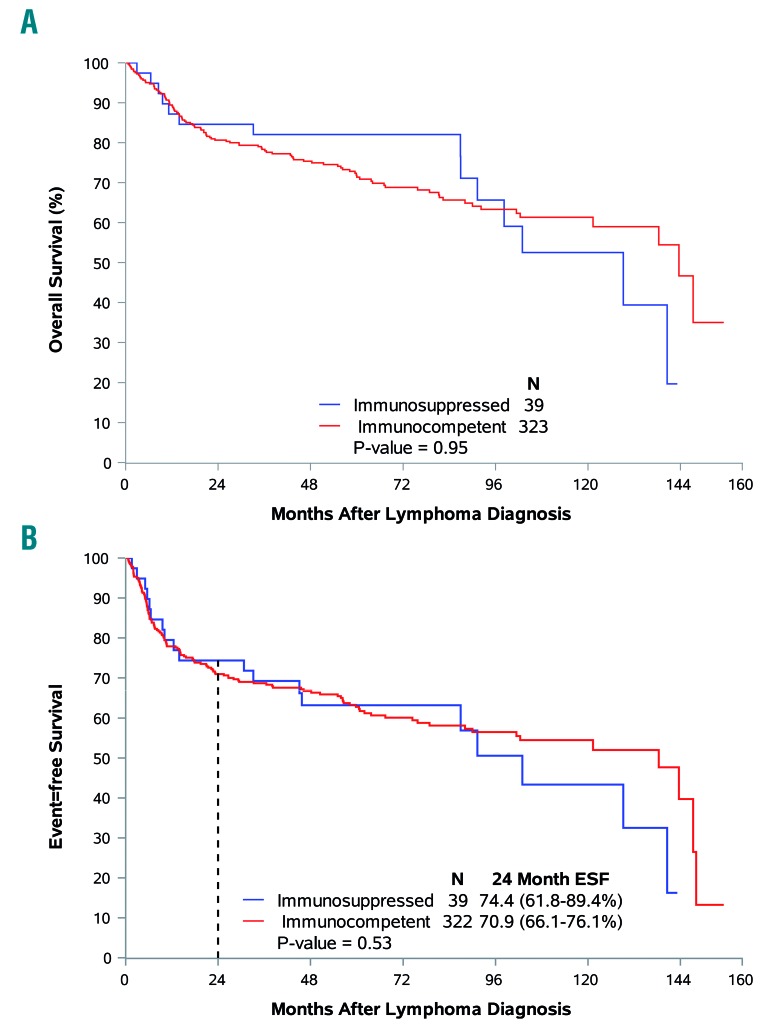
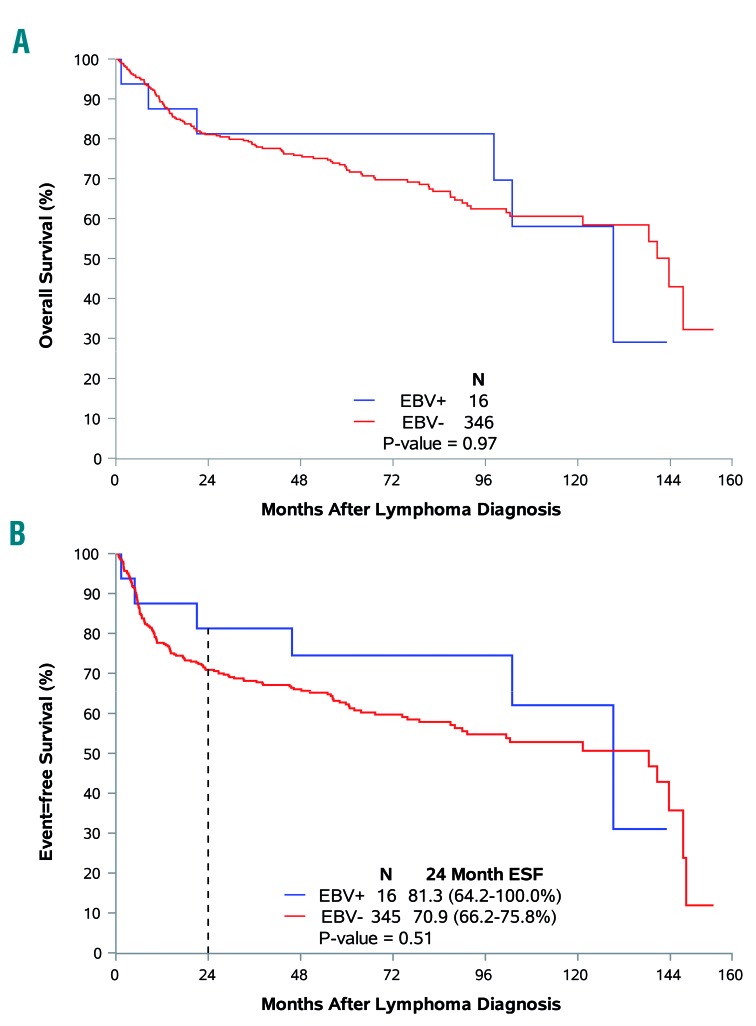
The prevalence, presenting clinical and pathological characteristics, and outcomes for patients with diffuse large B-cell lymphoma that is Epstein-Barr virus positive remain uncertain as does the impact of congenital or iatrogenic immunosuppression. Patients with newly diagnosed diffuse large B-cell lymphoma with available tissue arrays were identified from the University of Iowa/Mayo Clinic Molecular Epidemiology Resource. Patients infected with human immunodeficiency virus or who had undergone a prior organ transplant were excluded. Epstein-Barr virus-associated ribonucleic acid testing was performed on all tissue arrays. A history of significant congenital or iatrogenic immunosuppression was determined for all patients. At enrollment, 16 of the 362 (4.4%) biopsies were positive for Epstein-Barr virus. Thirty-nine (10.8%) patients had a significant history of immunosuppression. Patients with Epstein-Barr-positive diffuse large B-cell lymphoma had no unique clinical characteristics but on pathology exhibited a higher frequency of CD30 positivity (25.0% 8.1%, respectively; <0.01), and non-germinal-center subtype (62.5% 34.1%, respectively; <0.01). No baseline clinical characteristics were associated with a history of immunosuppression. With a median follow up of 59 months, and after adjustment for International Prognostic Index, there was no association of Epstein-Barr virus positivity or immunosuppression with event-free survival at 24 months (odds ratio=0.49; 95% confidence interval: 0.13-1.84 and odds ratio=0.81; 95% confidence interval: 0.37-1.77) or overall survival (hazard ratio=0.86; 95% confidence interval: 0.38-1.97 and hazard ratio=1.00; 95% confidence interval: 0.57-1.74). In contrast to non-Western populations, our North American population had a low prevalence of Epstein-Barr virus-positive diffuse large B-cell lymphoma that did not convey an adverse prognosis. A history of immunosuppression, while known to be a risk factor for the development of diffuse large B-cell lymphoma, did not affect subsequent prognosis.
EB 病毒阳性弥漫性大 B 细胞淋巴瘤的流行情况、临床表现和病理特征以及先天性或医源性免疫抑制的影响仍不确定。从爱荷华大学/梅奥诊所分子流行病学资源中确定了具有可用组织阵列的新发弥漫性大 B 细胞淋巴瘤患者。排除了感染人类免疫缺陷病毒或接受过先前器官移植的患者。对所有组织阵列均进行了 EBV 相关 RNA 检测。确定了所有患者的重大先天性或医源性免疫抑制史。在入组时,362 例活检中有 16 例(4.4%)为 EBV 阳性。39 例(10.8%)患者有重大免疫抑制史。EBV 阳性弥漫性大 B 细胞淋巴瘤患者无独特的临床特征,但在病理学上 CD30 阳性率更高(分别为 25.0%和 8.1%;<0.01),非生发中心亚型(分别为 62.5%和 34.1%;<0.01)。无基线临床特征与免疫抑制史相关。中位随访 59 个月,调整国际预后指数后,EBV 阳性或免疫抑制与 24 个月时无事件生存无关(优势比=0.49;95%置信区间:0.13-1.84 和优势比=0.81;95%置信区间:0.37-1.77)或总生存(风险比=0.86;95%置信区间:0.38-1.97 和风险比=1.00;95%置信区间:0.57-1.74)。与非西方人群不同,我们的北美人群中 EBV 阳性弥漫性大 B 细胞淋巴瘤的患病率较低,且预后不佳。免疫抑制史虽然是弥漫性大 B 细胞淋巴瘤发展的危险因素,但不影响后续预后。