Division of Thoracic Oncology, Shizuoka Cancer Center, 1007, Shimonagakubo, Nagaizumi-cho, Sunto-gun, Shizuoka, 411-8777, Japan.
Division of Rehabilitation Medicine, Shizuoka Cancer Center, 1007, Shimonagakubo, Nagaizumi-cho, Sunto-gun, Shizuoka, 411-8777, Japan.
BMC Cancer. 2017 Nov 28;17(1):800. doi: 10.1186/s12885-017-3795-2.
Cancer cachexia in elderly patients may substantially impact physical function and medical dependency. The aim of this study was to estimate the impact of cachexia on activity of daily living (ADL), length of hospital stay, and inpatient medical costs among elderly patients with advanced non-small-cell lung cancer (NSCLC) receiving chemotherapy.
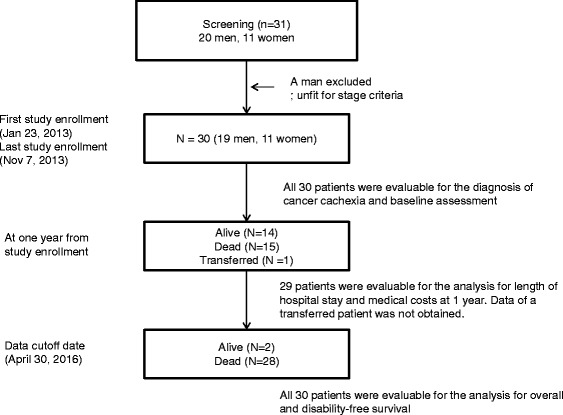
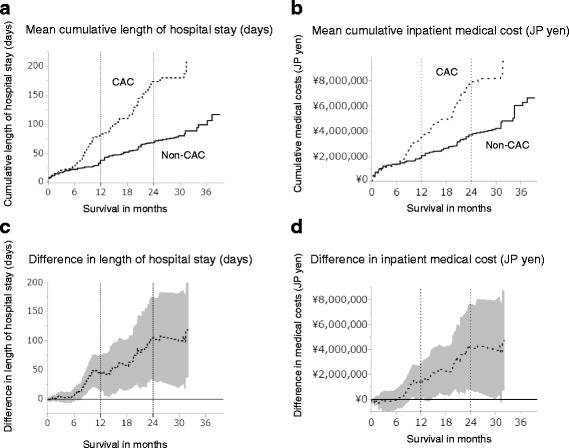
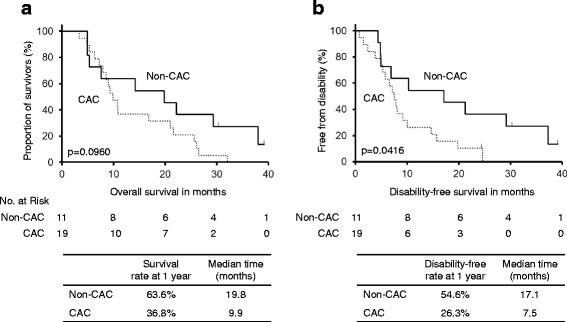
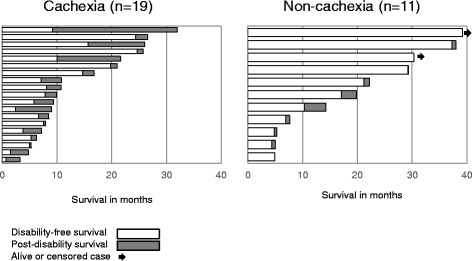
Thirty patients aged ≥70 years with advanced NSCLC (stage III-IV) scheduled to receive first-line chemotherapy were prospectively enrolled between January 2013 and November 2014. ADL was assessed using the Barthel index. The disability-free survival time (DFS) was calculated as the time between the date of study entry and the date of onset of a disabling event, which was defined as a 10-point decrease in the Barthel index from that at baseline. The mean cumulative function of the length of hospital stay and inpatient medical costs (¥, Japanese yen) was calculated.
The study patients comprised 11 women and 19 men, with a median age of 74 (range, 70-82) years. Cachexia was diagnosed in 19 (63%) patients. Cachectic patients had a shorter DFS (7.5 vs. 17.1 months, p < 0.05). During the first year from study entry, cachectic patients had longer cumulative lengths of hospital stay (80.7 vs. 38.5 days/person, p < 0.05), more frequent unplanned hospital visits or hospitalizations (4.2 vs. 1.7 times/person, p < 0.05), and higher inpatient medical costs (¥3.5 vs. ¥2.1 million/person, p < 0.05) than non-cachectic patients.
Elderly NSCLC patients with cachexia showed higher risks for disability, prolonged hospitalizations, and higher inpatient medical costs while receiving chemotherapy than patients without cachexia. Our results might indicate that there is a potential need for an early intervention to minimize progression to or development of cachexia, improve functional prognosis, and reduce healthcare resource burden in this population.
Trial registration number: UMIN000009768 . Name of registry: UMIN (University hospital Medical Information Network). Date of registration: 14 January 2013. Date of enrolment of the first participant to the trial: 23 January 2013.
老年癌症恶病质患者的身体机能和对医疗的依赖可能会受到严重影响。本研究旨在评估恶病质对接受化疗的老年晚期非小细胞肺癌(NSCLC)患者日常生活活动能力(ADL)、住院时间和住院医疗费用的影响。
2013 年 1 月至 2014 年 11 月,前瞻性纳入 30 名年龄≥70 岁、接受一线化疗的晚期 NSCLC(III-IV 期)患者。ADL 采用巴氏指数评估。无残疾生存时间(DFS)定义为基线时的巴氏指数下降 10 分。从研究入组日期到残疾事件发生日期的时间计算残疾无进展生存时间。计算住院时间和住院医疗费用(日元)的累积功能平均值。
本研究共纳入 11 名女性和 19 名男性患者,中位年龄为 74 岁(范围:70-82 岁)。19 名(63%)患者诊断为恶病质。恶病质患者的 DFS 更短(7.5 个月 vs. 17.1 个月,p<0.05)。从研究入组开始的第一年,恶病质患者的累积住院时间更长(80.7 天/人 vs. 38.5 天/人,p<0.05),更频繁地出现非计划门诊或住院(4.2 次/人 vs. 1.7 次/人,p<0.05),住院医疗费用更高(3500 万日元 vs. 2100 万日元/人,p<0.05)。
与非恶病质患者相比,接受化疗的老年 NSCLC 伴恶病质患者残疾风险更高,住院时间延长,住院医疗费用增加。这些结果可能表明,对于这一人群,存在潜在的需要进行早期干预以尽量减少恶病质的进展或发展,改善功能预后,并减轻医疗资源负担。
试验注册号:UMIN000009768。注册机构名称:UMIN(大学医院医疗信息网络)。注册日期:2013 年 1 月 14 日。试验入组的第一个参与者的注册日期:2013 年 1 月 23 日。