Delabranche Xavier, Helms Julie, Meziani Ferhat
Université de Strasbourg, Faculté de Médecine & Hôpitaux Universitaires de Strasbourg, Service de Réanimation, Nouvel Hôpital Civil, Strasbourg, France.
INSERM (French National Institute of Health and Medical Research), UMR 1260, Regenerative Nanomedicine (RNM), FMTS, Université de Strasbourg, Strasbourg, France.
Ann Intensive Care. 2017 Dec 2;7(1):117. doi: 10.1186/s13613-017-0339-5.
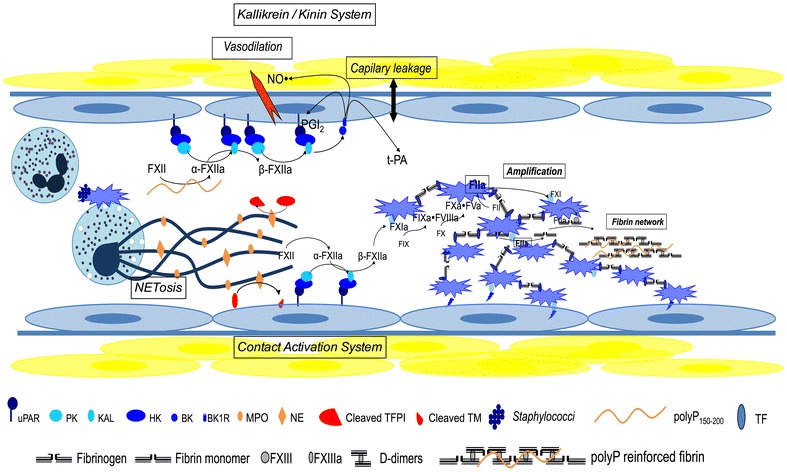
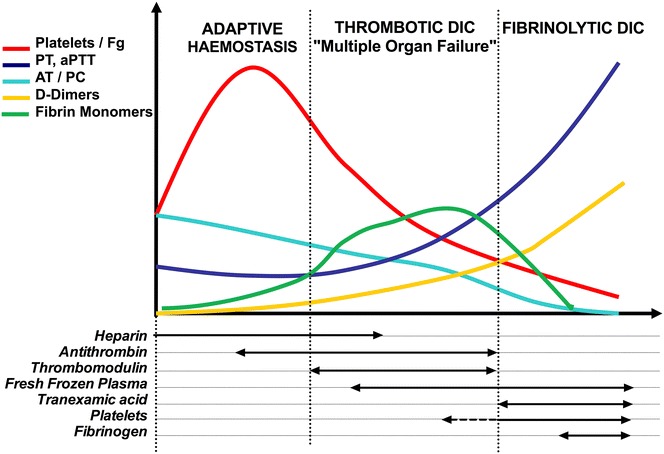
Host infection by a micro-organism triggers systemic inflammation, innate immunity and complement pathways, but also haemostasis activation. The role of thrombin and fibrin generation in host defence is now recognised, and thrombin has become a partner for survival, while it was seen only as one of the "principal suspects" of multiple organ failure and death during septic shock. This review is first focused on pathophysiology. The role of contact activation system, polyphosphates and neutrophil extracellular traps has emerged, offering new potential therapeutic targets. Interestingly, newly recognised host defence peptides (HDPs), derived from thrombin and other "coagulation" factors, are potent inhibitors of bacterial growth. Inhibition of thrombin generation could promote bacterial growth, while HDPs could become novel therapeutic agents against pathogens when resistance to conventional therapies grows. In a second part, we focused on sepsis-induced coagulopathy diagnostic challenge and stratification from "adaptive" haemostasis to "noxious" disseminated intravascular coagulation (DIC) either thrombotic or haemorrhagic. Besides usual coagulation tests, we discussed cellular haemostasis assessment including neutrophil, platelet and endothelial cell activation. Then, we examined therapeutic opportunities to prevent or to reduce "excess" thrombin generation, while preserving "adaptive" haemostasis. The fail of international randomised trials involving anticoagulants during septic shock may modify the hypothesis considering the end of haemostasis as a target to improve survival. On the one hand, patients at low risk of mortality may not be treated to preserve "immunothrombosis" as a defence when, on the other hand, patients at high risk with patent excess thrombin and fibrin generation could benefit from available (antithrombin, soluble thrombomodulin) or ongoing (FXI and FXII inhibitors) therapies. We propose to better assess coagulation response during infection by an improved knowledge of pathophysiology and systematic testing including determination of DIC scores. This is one of the clues to allocate the right treatment for the right patient at the right moment.
微生物对宿主的感染会引发全身炎症、固有免疫和补体途径,同时也会激活止血过程。凝血酶和纤维蛋白生成在宿主防御中的作用现已得到认可,凝血酶已成为生存的伙伴,而它曾仅被视为脓毒性休克期间多器官功能衰竭和死亡的“主要嫌疑对象”之一。本综述首先聚焦于病理生理学。接触激活系统、多磷酸盐和中性粒细胞胞外陷阱的作用已显现,提供了新的潜在治疗靶点。有趣的是,新发现的源自凝血酶和其他“凝血”因子的宿主防御肽(HDPs)是细菌生长的强效抑制剂。抑制凝血酶生成可能会促进细菌生长,而当对传统疗法产生耐药性时,HDPs可能会成为对抗病原体的新型治疗药物。在第二部分中,我们聚焦于脓毒症诱导的凝血病的诊断挑战以及从“适应性”止血到“有害的”血栓性或出血性弥散性血管内凝血(DIC)的分层。除了常规凝血检测外,我们还讨论了细胞止血评估,包括中性粒细胞、血小板和内皮细胞的激活。然后,我们研究了预防或减少“过量”凝血酶生成同时保留“适应性”止血的治疗机会。脓毒性休克期间涉及抗凝剂的国际随机试验失败可能会改变将止血终点作为改善生存靶点的假设。一方面,低死亡风险的患者可能无需治疗以保留“免疫血栓形成”作为一种防御,而另一方面,高风险且存在过量凝血酶和纤维蛋白生成的患者可能会从现有(抗凝血酶、可溶性血栓调节蛋白)或正在进行研究的(因子XI和因子XII抑制剂)治疗中获益。我们建议通过更好地了解病理生理学和进行包括DIC评分测定在内的系统检测,来更好地评估感染期间的凝血反应。这是在正确的时间为正确的患者分配正确治疗的线索之一。