Department of Pediatrics, Cincinnati Children's Hospital Medical Center, Cincinnati, OH.
Department of Pathology and Immunology, Washington University School of Medicine and St. Louis Children's Hospital, St. Louis, MO.
J Pediatr. 2018 Mar;194:158-164.e1. doi: 10.1016/j.jpeds.2017.10.026. Epub 2017 Dec 1.
To describe disease course, histopathology, and outcomes for infants with atypical presentations of alveolar capillary dysplasia with misalignment of the pulmonary veins (ACDMPV) who underwent bilateral lung transplantation.
We reviewed clinical history, diagnostic studies, explant histology, genetic sequence results, and post-transplant course for 6 infants with atypical ACDMPV who underwent bilateral lung transplantation at St. Louis Children's Hospital. We compared their histology with infants with classic ACDMPV and compared their outcomes with infants transplanted for other indications.
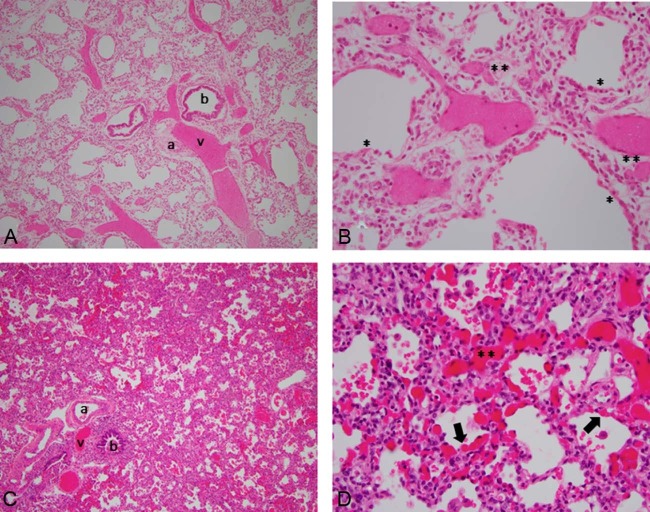
In contrast with neonates with classic ACDPMV who present with severe hypoxemia and refractory pulmonary hypertension within hours of birth, none of the infants with atypical ACDMPV presented with progressive neonatal respiratory failure. Three infants had mild neonatal respiratory distress and received nasal cannula oxygen. Three other infants had no respiratory symptoms at birth and presented with hypoxemia and pulmonary hypertension at 2-3 months of age. Bilateral lung transplantation was performed at 4-20 months of age. Unlike in classic ACDMPV, histopathologic findings were not distributed uniformly and were not diffuse. Three subjects had apparent nonmosaic genetic defects involving FOXF1. Two infants had extrapulmonary anomalies (posterior urethral valves, inguinal hernia). Three transplanted children are alive at 5-16 years of age, similar to outcomes for infants transplanted for other indications. Lung explants from infants with atypical ACDMPV demonstrated diagnostic but nonuniform histopathologic findings.
The 1- and 5-year survival rates for infants with atypical ACDMPV are similar to infants transplanted for other indications. Given the clinical and histopathologic spectra, ACDMPV should be considered in infants with hypoxemia and pulmonary hypertension, even beyond the newborn period.
描述接受双侧肺移植的具有肺静脉错位的肺泡毛细血管发育不良(ACDMPV)不典型表现的婴儿的疾病过程、组织病理学和结局。
我们回顾了在圣路易斯儿童医院接受双侧肺移植的 6 例具有不典型 ACDMPV 的婴儿的临床病史、诊断研究、移植肺组织病理学、基因序列结果和移植后病程。我们将他们的组织病理学与经典 ACDMPV 婴儿进行了比较,并将他们的结局与因其他适应症接受移植的婴儿进行了比较。
与出生后数小时内出现严重低氧血症和难治性肺动脉高压的新生儿期经典 ACDPMV 患儿不同,不典型 ACDMPV 患儿均无进行性新生儿呼吸衰竭表现。3 例婴儿有轻度新生儿呼吸窘迫,接受鼻塞吸氧。其他 3 例婴儿出生时无呼吸症状,2-3 个月时出现低氧血症和肺动脉高压。4-20 个月时进行双侧肺移植。与经典 ACDMPV 不同,组织病理学发现并非均匀分布,也非弥漫性。3 例患儿存在明显的非嵌合性 FOXF1 基因缺陷。2 例患儿有肺外异常(后尿道瓣膜、腹股沟疝)。3 例移植儿童在 5-16 岁时存活,与因其他适应症接受移植的婴儿结局相似。不典型 ACDMPV 婴儿的移植肺组织显示出诊断性但非均匀的组织病理学发现。
不典型 ACDMPV 婴儿的 1 年和 5 年生存率与因其他适应症接受移植的婴儿相似。鉴于临床表现和组织病理学谱,即使在新生儿期之后,也应考虑 ACDMPV 作为低氧血症和肺动脉高压婴儿的诊断。