Division of Gastroenterology and Hepatology, Department of Medicine, University of California, San Francisco, San Francisco, California.
Department of Public Health Sciences, Medical University of South Carolina, Charleston, South Carolina.
Clin Gastroenterol Hepatol. 2018 Jun;16(6):936-946. doi: 10.1016/j.cgh.2017.11.042. Epub 2017 Dec 2.
BACKGROUND & AIMS: Acetaminophen overdose is the leading cause of acute liver injury (ALI) and acute liver failure (ALF) in the developed world. Sex differences in acetaminophen-induced hepatotoxicity have not been described.
We collected data from the Acute Liver Failure Study Group cohort, a national registry of 32 academic medical centers in North America of adults with ALI or ALF, including 1162 patients with acetaminophen-induced ALI (n = 250) or acetaminophen-induced ALF (n = 912) from January 2000 through September 2016. We analyzed data on patient presentation, disease course, demographics, medical and psychiatric history, medication use, substance use, and details of acetaminophen ingestion. Sex differences in continuous and categorical variables were evaluated by Wilcoxon rank-sum and χ analysis or the Fisher exact test. Our primary aim was to evaluate sex differences in the presentation and clinical course of acetaminophen-induced acute liver injury or liver failure, and our secondary goal was to compare overall and transplant-free survival between sexes.
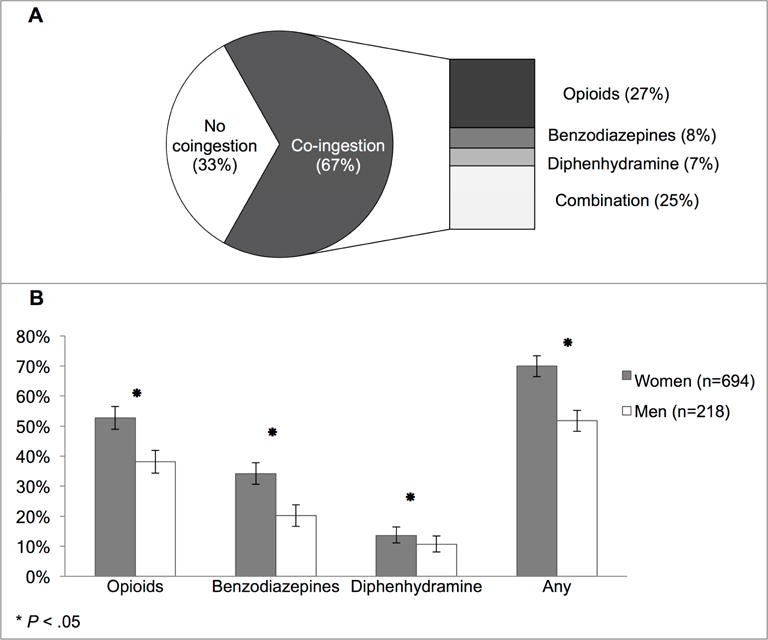
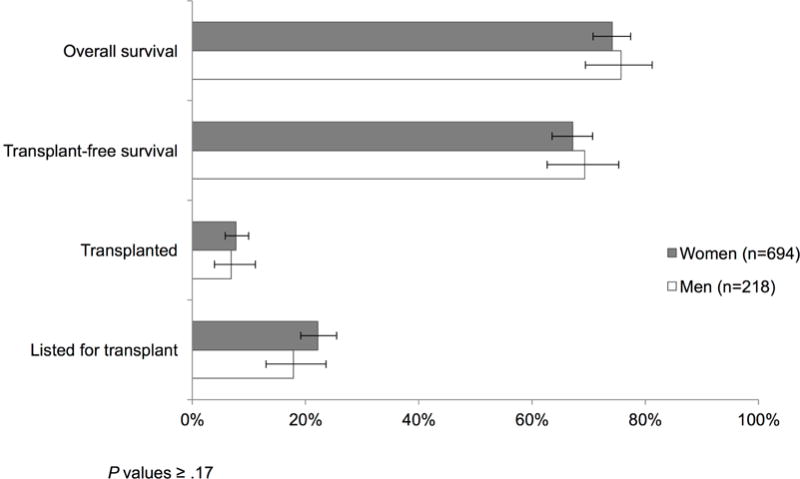
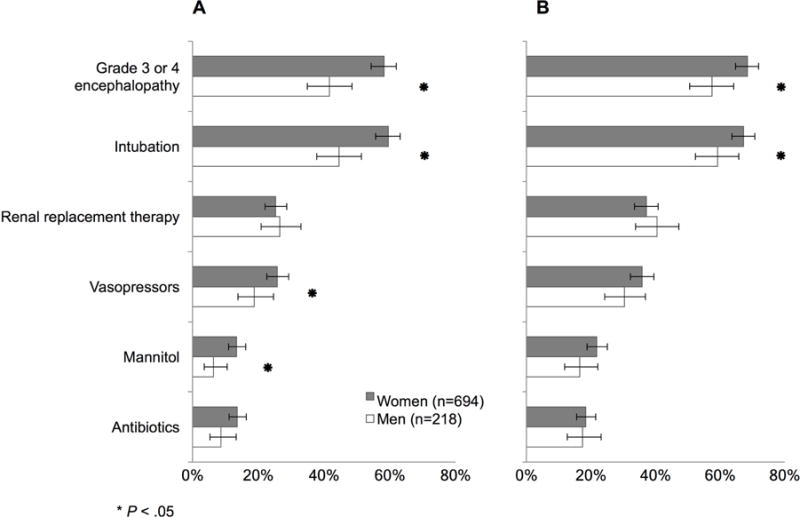
Most patients with acetaminophen-induced ALI (68%) or ALF (76%) were women. Higher proportions of women than men had psychiatric disease (60% of women vs 48% of men, P < .01) and had co-ingestion with sedating agents (70% of women vs 52% of men, P < .01)-more than half of which were opioids. Higher proportions of women had severe hepatic encephalopathy (HE) (68% of women vs 58% of men), and required intubation (67% of women vs 59% of men, P values <.03). Higher proportions of women used vasopressors (26% of women vs 19% of men, P = .04) or mannitol (13% of women vs 6% of men, P < .01); proportions of male vs female patients with transplant-free survival were similar (68%). On adjusted analysis, women had higher risk of severe HE (adjusted odds ratio [AOR], 1.66; 95% CI, 1.17-2.35). We found a significant interaction between sex and co-ingestion of sedating agents (P < .01); co-ingestion increased odds of severe HE in women 2-fold (AOR, 1.86; 95% CI, 1.28-2.69; P < .01) but not in men (AOR; 0.62; 95% CI, 0.34-1.13; P = .12).
In an analysis of the Acute Liver Failure Study Group cohort, we found acetaminophen-induced ALI and ALF to be more common among women. Women have greater critical care needs than men, and increased risk for severe HE, which could be due in part to increased use of sedatives. Future studies should investigate sex differences in acetaminophen metabolism and hepatotoxicity, particularly among users of opioids.
在发达国家,对乙酰氨基酚过量是急性肝损伤(ALI)和急性肝衰竭(ALF)的主要原因。对乙酰氨基酚诱导的肝毒性的性别差异尚未描述。
我们从北美 32 家学术医疗中心的急性肝衰竭研究组队列中收集数据,该队列是一个包括 ALI 或 ALF 成年患者的全国登记处,包括 2000 年 1 月至 2016 年 9 月期间的 1162 例乙酰氨基酚诱导的 ALI(n=250)或乙酰氨基酚诱导的 ALF(n=912)患者。我们分析了患者表现、疾病过程、人口统计学、医疗和精神病史、药物使用、物质使用以及对乙酰氨基酚摄入的详细信息。通过 Wilcoxon 秩和检验或 χ 检验或 Fisher 确切检验评估连续和分类变量的性别差异。我们的主要目的是评估对乙酰氨基酚诱导的急性肝损伤或肝衰竭的表现和临床过程中的性别差异,我们的次要目标是比较性别之间的总生存率和无移植生存率。
大多数乙酰氨基酚诱导的 ALI(68%)或 ALF(76%)患者为女性。与男性相比,更多的女性有精神疾病(60%的女性比 48%的男性,P <.01)和合用镇静剂(70%的女性比 52%的男性,P <.01),其中一半以上是阿片类药物。更多的女性有严重的肝性脑病(HE)(68%的女性比 58%的男性),需要插管(67%的女性比 59%的男性,P 值<.03)。更多的女性使用血管加压素(26%的女性比 19%的男性,P =.04)或甘露醇(13%的女性比 6%的男性,P <.01);无移植生存率的男性和女性患者比例相似(68%)。在调整分析中,女性发生严重 HE 的风险更高(调整后的优势比[AOR],1.66;95%CI,1.17-2.35)。我们发现性别和合用镇静剂之间存在显著的交互作用(P <.01);合用镇静剂使女性发生严重 HE 的风险增加了两倍(AOR,1.86;95%CI,1.28-2.69;P <.01),而男性则没有(AOR;0.62;95%CI,0.34-1.13;P=.12)。
在对急性肝衰竭研究组队列的分析中,我们发现乙酰氨基酚诱导的 ALI 和 ALF 在女性中更为常见。女性比男性需要更多的重症监护,并且发生严重 HE 的风险更高,这可能部分归因于镇静剂的使用增加。未来的研究应调查对乙酰氨基酚代谢和肝毒性的性别差异,特别是在阿片类药物使用者中。