Department of Surgery, Amphia Hospital, Breda.
Department of Vascular Surgery, Erasmus University Medical Center, Rotterdam.
Clin Interv Aging. 2017 Nov 22;12:1985-1992. doi: 10.2147/CIA.S137570. eCollection 2017.
Owing to the aging population, the number of elderly patients with critical limb ischemia (CLI) has increased. The consequence of amputation is immense. However, at the moment, information about the mortality after amputation in the elderly vascular patients is unknown. For this reason, this study evaluated mortality rates and patient-related factors associated with mortality after a major amputation in elderly patients with CLI.
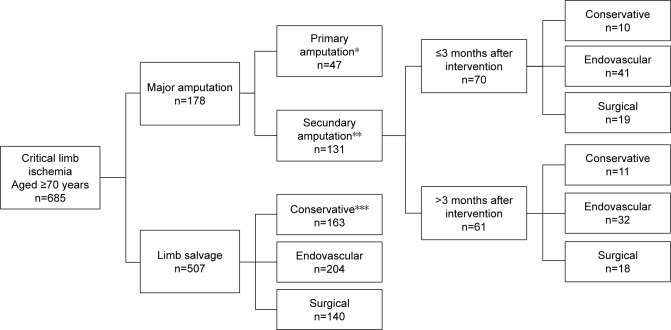
From 2006 to 2013, we included patients aged >70 years who were treated for chronic CLI by primary or secondary major amputation within or after 3 months of initial therapy (revascularization or conservative management). Outcome measurements were mortality after major amputation and factors associated with mortality (age, comorbidity and timing of amputation).
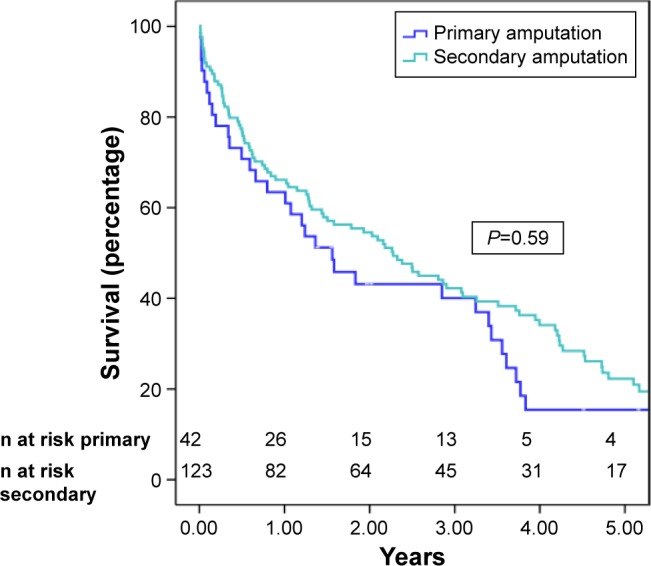
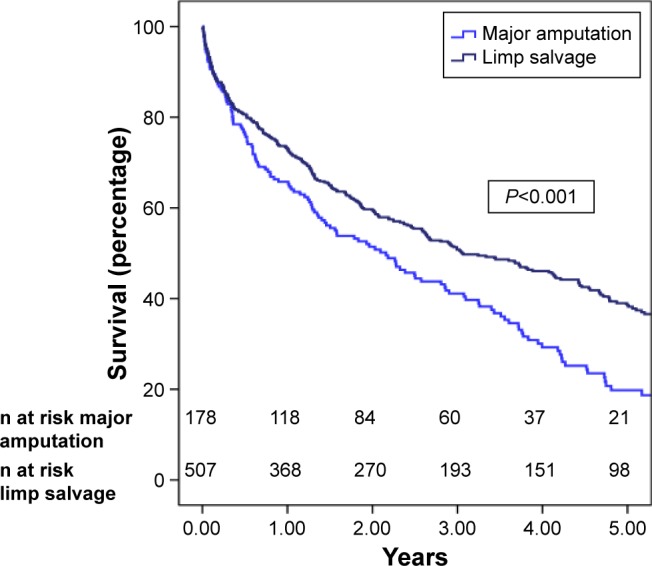
In total, 168/651 patients (178 legs; 26%) underwent a major amputation. Patients were stratified by age: 70-80 years (n=86) and >80 years (n=82). Overall mortality after major amputation was 44%, 66% and 85% after 1, 3 and 5 years, respectively. The 6-month and 1-year mortality in patients aged 80 years or older was, respectively, 59% or 63% after a secondary amputation <3 months versus 34% and 44% after a secondary amputation >3 months. Per year of age, the mortality rate increased by 4% (=0.005). No significant difference in mortality after major amputation was found in the presence of comorbidity or according to Rutherford classification.
Despite developments in the treatment of CLI by revascularization, amputation rates remain high and are associated with tremendous mortality rates. Secondary amputation after a failed attempt of revascularization causes a higher mortality. Further research concerning timing of amputation and patient-related outcome is needed to evaluate if selected patients might benefit from primary amputation.
由于人口老龄化,患有严重肢体缺血(CLI)的老年患者数量有所增加。截肢的后果是巨大的。然而,目前,关于老年血管患者截肢后死亡率的信息尚不清楚。出于这个原因,本研究评估了 CLI 老年患者经初次治疗(血运重建或保守治疗)后 3 个月内或之后初次治疗时主要截肢后死亡率和与死亡率相关的患者相关因素。
2006 年至 2013 年,我们纳入了年龄>70 岁的患者,这些患者因慢性 CLI 接受了初次治疗(血运重建或保守治疗)后或 3 个月内进行了主要的或次要的截肢。主要截肢后死亡率和与死亡率相关的因素(年龄、合并症和截肢时间)。
共有 168/651 例患者(178 条腿;26%)接受了主要截肢。患者按年龄分层:70-80 岁(n=86)和>80 岁(n=82)。主要截肢后总体死亡率分别为 1 年、3 年和 5 年后的 44%、66%和 85%。年龄在 80 岁或以上的患者,初次治疗后 3 个月内进行二次次要截肢的 6 个月和 1 年死亡率分别为 59%或 63%,而初次治疗后 3 个月内进行二次次要截肢的 34%和 44%。每年增加 4%(=0.005)。合并症的存在或根据 Rutherford 分类,在主要截肢后死亡率没有显著差异。
尽管通过血运重建治疗 CLI 有所发展,但截肢率仍然很高,且与极高的死亡率相关。血运重建失败后进行二次次要截肢会导致更高的死亡率。需要进一步研究截肢时机和患者相关结局,以评估是否可以选择某些患者从初次截肢中获益。