Pós Graduação de Ciências da Saúde, Pontifícia Universidade Católica do Paraná, Rua Imaculada Conceição, 1155 - Parque Tecnológico 06, Curitiba, Paraná, CEP: 80.215-901, Brazil.
Department of Epidemiology, Erasmus MC, Erasmus MC, University Medical Center Rotterdam Office Na 29-16, PO Box 2040, 3000, CA, Rotterdam, The Netherlands.
BMC Geriatr. 2017 Dec 5;17(1):279. doi: 10.1186/s12877-017-0672-4.
It remains unclear into which level the systolic blood pressure (SBP) should be lowered in order to provide the best cardiovascular protection among older people. Hypertension guidelines recommendation on attaining SBP levels <150 mmHg in this population is currently based on experts' opinion. To clarify this issue, we systematically reviewed and quantified available evidence on the impact of achieving different SBP levels <150 mmHg on various adverse outcomes in subjects aged ≥60 years old receiving antihypertensive drug treatment.
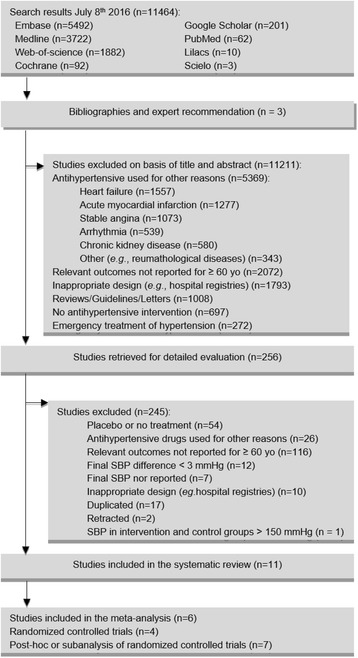
We searched 8 databases to identify randomized controlled trials (RCTs) and post-hoc analyses or subanalyses of RCTs reporting the effects of attaining different SBP levels <150 mmHg on the risk of stroke, acute myocardial infarction, heart failure, cardiovascular mortality and all-cause mortality in participants aged ≥60 years. We performed random-effects meta-analyses stratified by study design.
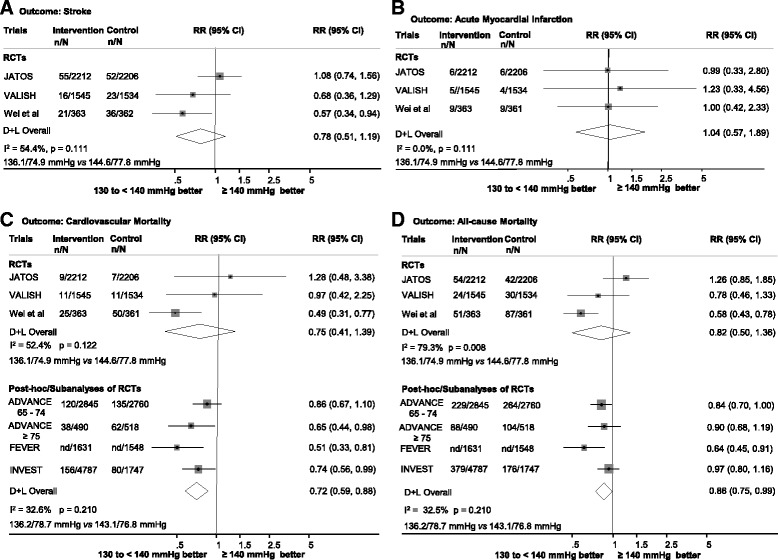
Eleven studies (> 33,600 participants) were included. Compared with attaining SBP levels ≥140 mmHg, levels of 130 to <140 mmHg were not associated with lower risk of outcomes in the meta-analysis of RCTs, whereas there was an associated reduction of cardiovascular mortality (RR 0.72, 95% CI 0.59-0.88) and all-cause mortality (RR 0.86, 95% CI 0.75-0.99) in the meta-analysis of post-hoc analyses or subanalyses of RCTs. Limited and conflicting data were available for the SBP levels of <130 mmHg and 140 to <150 mmHg.
Among older people, there is suggestive evidence that achieving SBP levels of 130 to <140 mmHg is associated with lower risks of cardiovascular and all-cause mortality. Future trials are required to confirm these findings and to provide additional evidence regarding the <130 and 140 to <150 mmHg SBP levels.
为了在老年人中提供最佳心血管保护,收缩压(SBP)应降至何种水平仍不清楚。高血压指南建议在该人群中达到 SBP 水平<150mmHg,目前基于专家意见。为了澄清这一问题,我们系统地回顾和量化了现有的证据,以了解在接受抗高血压药物治疗的年龄≥60 岁的受试者中,达到不同的 SBP 水平<150mmHg 对各种不良结局的影响。
我们搜索了 8 个数据库,以确定报告了达到不同的 SBP 水平<150mmHg 对年龄≥60 岁的参与者中风、急性心肌梗死、心力衰竭、心血管死亡率和全因死亡率风险影响的随机对照试验(RCT)和事后分析或 RCT 的亚分析。我们按研究设计进行了随机效应荟萃分析。
纳入了 11 项研究(>33600 名参与者)。与达到 SBP 水平≥140mmHg 相比,荟萃分析中的 RCT 表明,达到 130 至<140mmHg 的 SBP 水平与较低的结局风险无关,而在 RCT 的事后分析或亚分析的荟萃分析中,心血管死亡率(RR0.72,95%CI0.59-0.88)和全因死亡率(RR0.86,95%CI0.75-0.99)均有降低。对于 SBP 水平<130mmHg 和 140 至<150mmHg,可用的数据有限且存在矛盾。
在老年人中,有证据表明达到 130 至<140mmHg 的 SBP 水平与较低的心血管和全因死亡率风险相关。需要进一步的试验来证实这些发现,并提供关于<130mmHg 和 140 至<150mmHg SBP 水平的额外证据。