Department of Thoracic Surgery, Hangzhou Red Cross Hospital, Hangzhou, Zhejiang, China.
PLoS One. 2017 Dec 6;12(12):e0188704. doi: 10.1371/journal.pone.0188704. eCollection 2017.
This study aimed to assess the diagnostic performance of Xpert MTB/RIF for tuberculous pericarditis (TBP) using pericardial tissues.
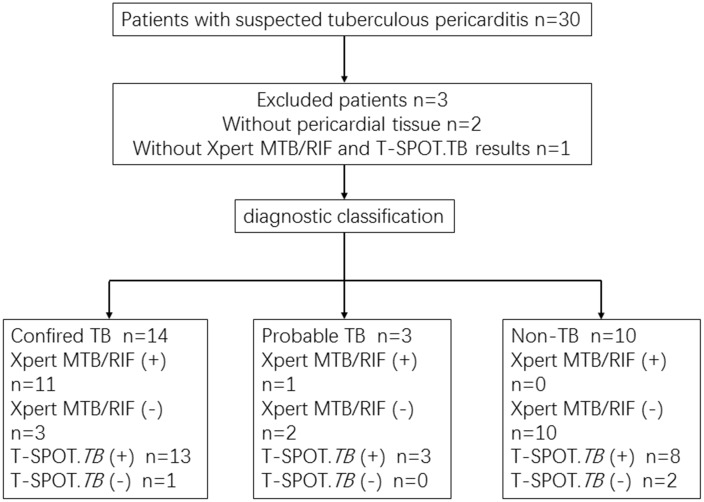
The study involved 30 patients admitted with suspected TBP from January-December 2016; three patients were later excluded. The interferon-γ release assay (T-SPOT.TB) and the Xpert MTB/RIF test were performed using peripheral blood and pericardial tissues, respectively. TBP was confirmed using pericardial histopathology and a composite reference standard (CRS). We analyzed the sensitivity, specificity, predictive value (PV), likelihood ratio (LR), and area under curve (AUC) of both assays.
Fourteen patients were confirmed as TBP, 10 as non-TBP, and 3 as probable TBP. The sensitivity, specificity, positive PV (PPV), negative PV (NPV), PLR, NLR, and AUC (95% confidence interval [CI]) of the Xpert MTB/RIF assay were 78.6% (49.2-95.3%) and 70.6% (44.0-89.7%); 92.3% (64.0-99.8%) and 100% (69.2-100%); 91.7% (61.5-99.8%) and 100% (73.5-100%); 80.0% (51.9-95.7%) and 66.7% (38.4-88.2%); 10.21 (1.52-68.49) and the PLR value was undefined with CRS as the reference; 0.23 (0.08-0.64) and 0.29(0.14-0.61); and 0.854 (0.666-0.959) and 0.853 (0.664-0.959), against histopathology and CRS, respectively. The sensitivity, specificity, PPV, NPV, PLR, NLR, and AUC values (95% CI) of T-SPOT.TB were 92.9% (66.1-99.8%) and 94.1% (71.3-99.9%); 15.4% (1.9-45.5%) and 20.0% (2.5-55.6%); 54.2% (32.8-74.5%) and 66.7% (44.7-84.4%); 66.7% (9.4-99.2%) and 66.7% (9.4-99.2%); 1.10 (0.83-1.44) and 1.18 (0.84-1.6); 0.46 (0.05-4.53) and 0.29 (0.03-2.85); and 0.541(0.340-0.733) and 0.571(0.367-0.758), against histopathology and CRS, respectively. The differences in sensitivity, PPV, and AUC of Xpert MTB/RIF and T-SPOT.TB were not statistically significant (P > 0.05), compared to those of histopathology and CRS. However, the differences in specificity and NPV of the two assays were significant (P < 0.05), compared to those of histopathology and CRS.
Xpert MTB/RIF test is a valid diagnostic technique for TBP with higher sensitivity and specificity than T-SPOT.TB.
本研究旨在评估 Xpert MTB/RIF 检测在结核性心包炎(TBP)诊断中的表现,采用心包组织样本进行检测。
研究纳入了 2016 年 1 月至 12 月期间因疑似 TBP 入院的 30 名患者,其中 3 名患者后来被排除。采用外周血和心包组织分别进行干扰素-γ释放试验(T-SPOT.TB)和 Xpert MTB/RIF 检测。心包组织病理学和综合参考标准(CRS)用于确诊 TBP。我们分析了两种检测方法的灵敏度、特异性、阳性预测值(PPV)、阴性预测值(NPV)、阳性似然比(PLR)、阴性似然比(NLR)和曲线下面积(AUC)。
最终 14 名患者被确诊为 TBP,10 名患者为非 TBP,3 名患者为可能的 TBP。Xpert MTB/RIF 检测的灵敏度、特异性、阳性 PPV、阴性 NPV、PLR、NLR 和 AUC(95%置信区间[CI])分别为 78.6%(49.2-95.3%)和 70.6%(44.0-89.7%);92.3%(64.0-99.8%)和 100%(69.2-100%);91.7%(61.5-99.8%)和 100%(73.5-100%);80.0%(51.9-95.7%)和 66.7%(38.4-88.2%);10.21(1.52-68.49)和 PLR 值未定义,以 CRS 为参考;0.23(0.08-0.64)和 0.29(0.14-0.61);0.854(0.666-0.959)和 0.853(0.664-0.959),分别与组织病理学和 CRS 相对应。T-SPOT.TB 的灵敏度、特异性、PPV、NPV、PLR、NLR 和 AUC 值(95%CI)分别为 92.9%(66.1-99.8%)和 94.1%(71.3-99.9%);15.4%(1.9-45.5%)和 20.0%(2.5-55.6%);54.2%(32.8-74.5%)和 66.7%(44.7-84.4%);66.7%(9.4-99.2%)和 66.7%(9.4-99.2%);1.10(0.83-1.44)和 1.18(0.84-1.6);0.46(0.05-4.53)和 0.29(0.03-2.85);0.541(0.340-0.733)和 0.571(0.367-0.758),分别与组织病理学和 CRS 相对应。Xpert MTB/RIF 和 T-SPOT.TB 与组织病理学和 CRS 相比,在灵敏度、PPV 和 AUC 方面的差异无统计学意义(P>0.05),但在特异性和 NPV 方面的差异有统计学意义(P<0.05)。
Xpert MTB/RIF 检测是一种有效的 TBP 诊断技术,其灵敏度和特异性均高于 T-SPOT.TB。