Kim Sung Han, Suh Yoon Seok, Lee Dong-Eun, Park Boram, Joo Jungnam, Joung Jae Young, Seo Ho Kyung, Lee Kang Hyun, Chung Jinsoo
Department of Urology, Center for Prostate Cancer, Research Institute and Hospital of National Cancer Center, Goyang, Korea.
Biometric Research Branch, Division of Cancer Epidemiology and Prevention, Research Institute and Hospital of National Cancer Center, Goyang, Korea.
Oncotarget. 2017 Sep 6;8(55):93633-93643. doi: 10.18632/oncotarget.20674. eCollection 2017 Nov 7.
The aim of this study was to compare progression-free survival (PFS) and overall survival (OS) between metachronous and synchronous metastatic renal cell carcinomas treated with VEGF-targeted therapy.
Between 2005 and 2014, 93 (78.8%) intermediate- and 25 (21.2%) poor-Heng-risk patients, including 32 (27.1%) patients with metachronous and 86 (72.9%) patients with synchronous renal cell carcinoma, were enrolled retrospectively. PFS and OS values were compared according to the number of risk factors and treatment-free interval using the Kaplan-Meier method and log-rank test. The prognostic risk factors were also evaluated using a Cox proportional hazard model, with a p-value < 0.05 indicating statistical significance.
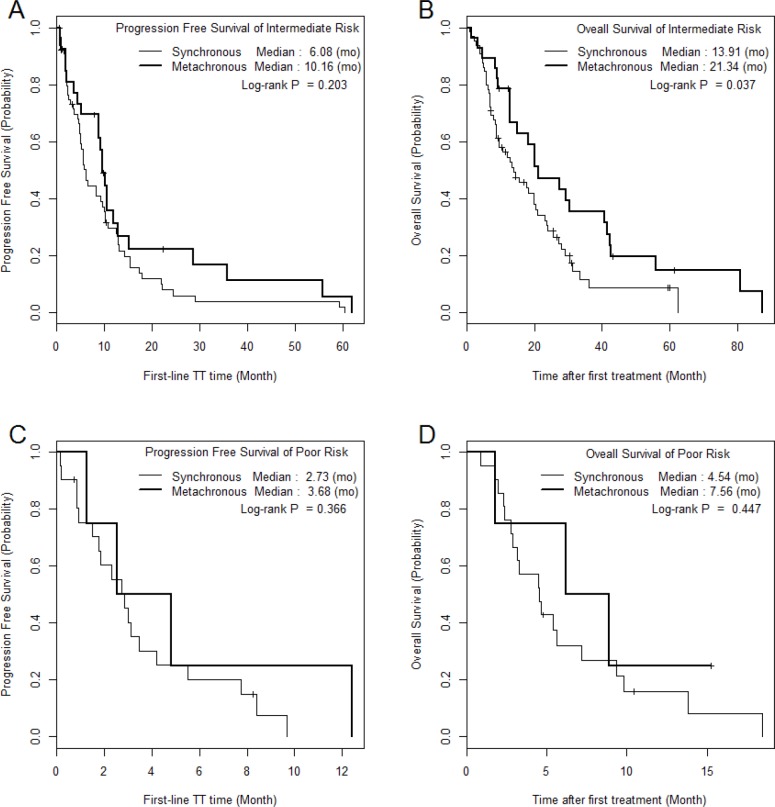
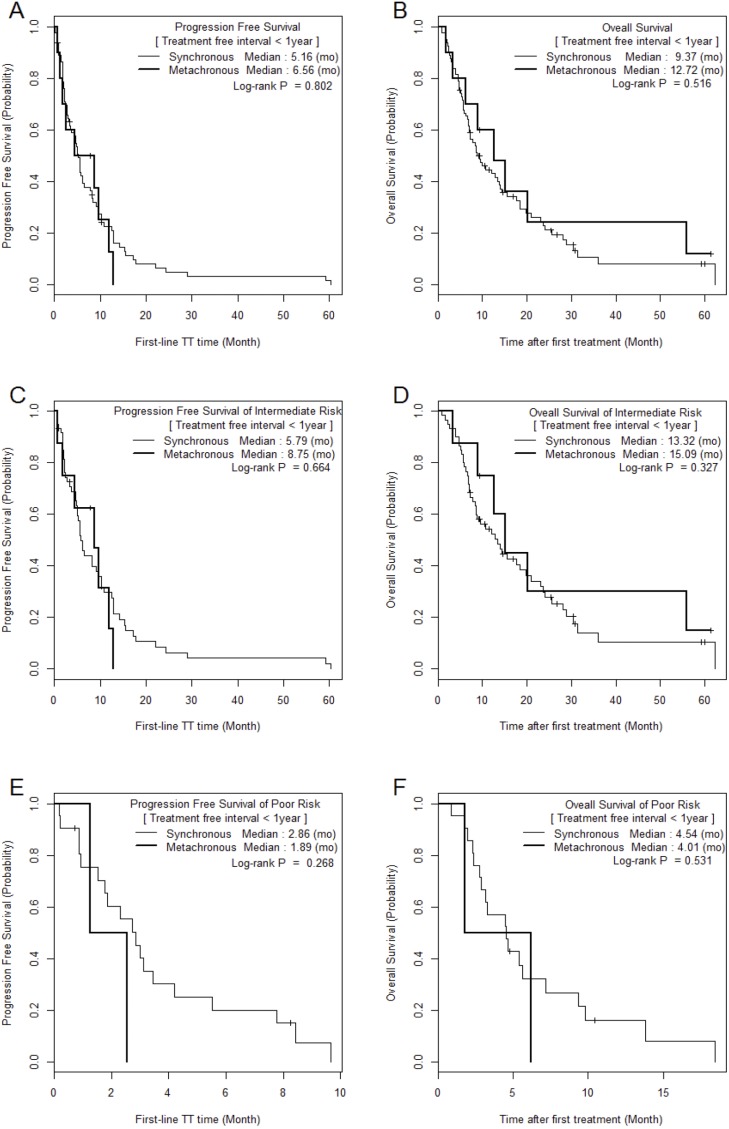
During a median 5.0-month treatment and 59.3-month follow-up, analysis of the PFS/OS of SM (5.2/9.6 months) and MM (9.6/20.1 months) yielded a significant difference in OS (p = 0.010). However, there was no significant difference when Heng risk groups and treatment-free interval were considered (p > 0.05). There was a significant difference in PFS (hazard ratio: 1.81) and OS (hazard ratio: 2.19) with increasing number of Heng risk factors among patients with synchronous renal cell carcinoma and a treatment-free interval <1 year. Metastatic type, anemia, and neutrophilia were significant predictive factors for OS in multivariable analysis (p < 0.05).
The metastatic type of renal cell carcinoma (synchronous or metachronous) significantly affects survival; metachronous type is associated with more favorable outcomes than synchronous type. However, after stratification according to Heng risk factors and treatment-free interval, the differences in survival between metachronous and synchronous type were insignificant.
本研究的目的是比较接受血管内皮生长因子(VEGF)靶向治疗的异时性和同时性转移性肾细胞癌的无进展生存期(PFS)和总生存期(OS)。
回顾性纳入了2005年至2014年间的93例(78.8%)中危和25例(21.2%)低危风险患者,其中包括32例(27.1%)异时性肾细胞癌患者和86例(72.9%)同时性肾细胞癌患者。使用Kaplan-Meier法和对数秩检验,根据风险因素数量和无治疗间期比较PFS和OS值。还使用Cox比例风险模型评估预后风险因素,p值<0.05表示具有统计学意义。
在中位5.0个月的治疗期和59.3个月的随访期内,对同时性转移(SM,5.2/9.6个月)和异时性转移(MM,9.6/20.1个月)的PFS/OS分析显示,OS存在显著差异(p = 0.010)。然而,在考虑低危风险组和无治疗间期时,没有显著差异(p>0.05)。对于同时性肾细胞癌且无治疗间期<1年的患者,随着低危风险因素数量的增加,PFS(风险比:1.81)和OS(风险比:2.19)存在显著差异。在多变量分析中,转移类型、贫血和中性粒细胞增多是OS的显著预测因素(p<0.05)。
肾细胞癌的转移类型(同时性或异时性)显著影响生存期;异时性类型比同时性类型的预后更有利。然而,根据低危风险因素和无治疗间期进行分层后,异时性和同时性类型之间的生存差异不显著。