Hematology Research Unit Helsinki, University of Helsinki and Department of Hematology, Helsinki University Hospital Comprehensive Cancer Center, Finland.
Department of Clinical Chemistry and Hematology, University of Helsinki, Finland.
Haematologica. 2018 Feb;103(2):304-312. doi: 10.3324/haematol.2017.175729. Epub 2017 Dec 7.
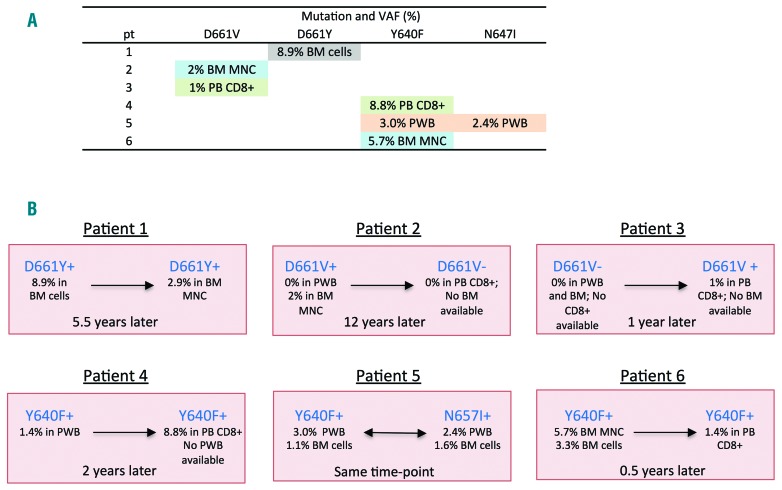
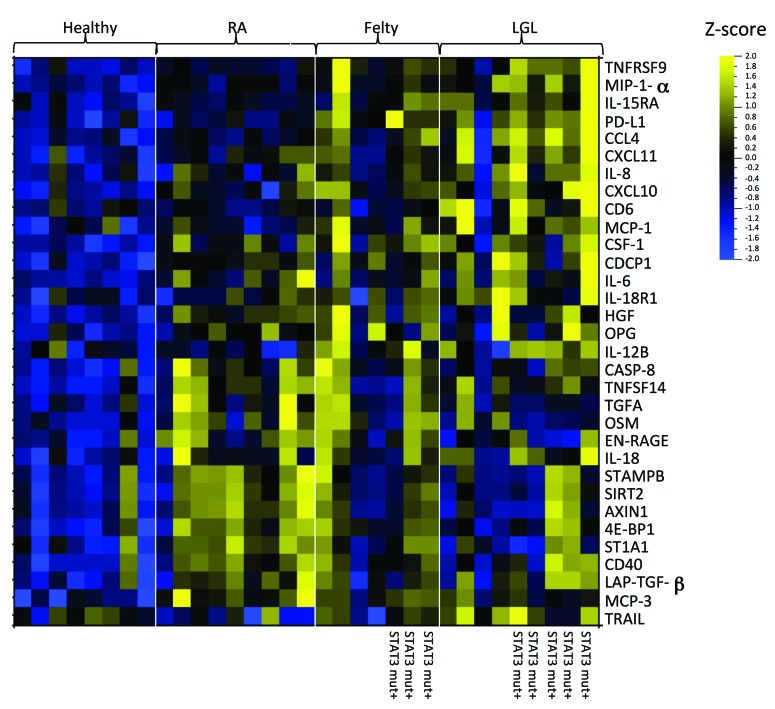
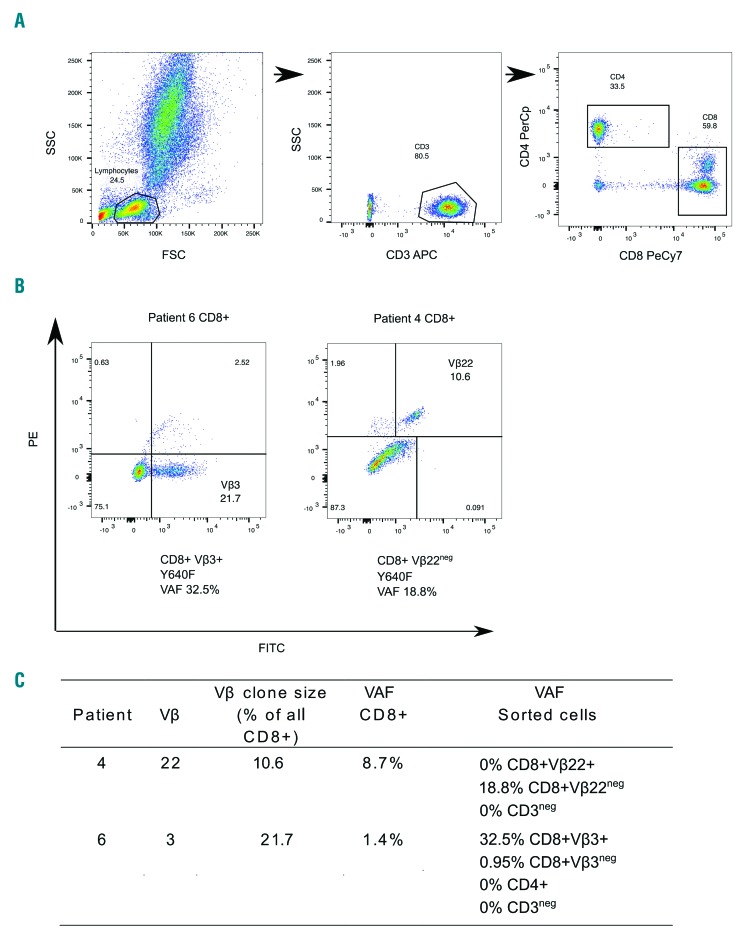
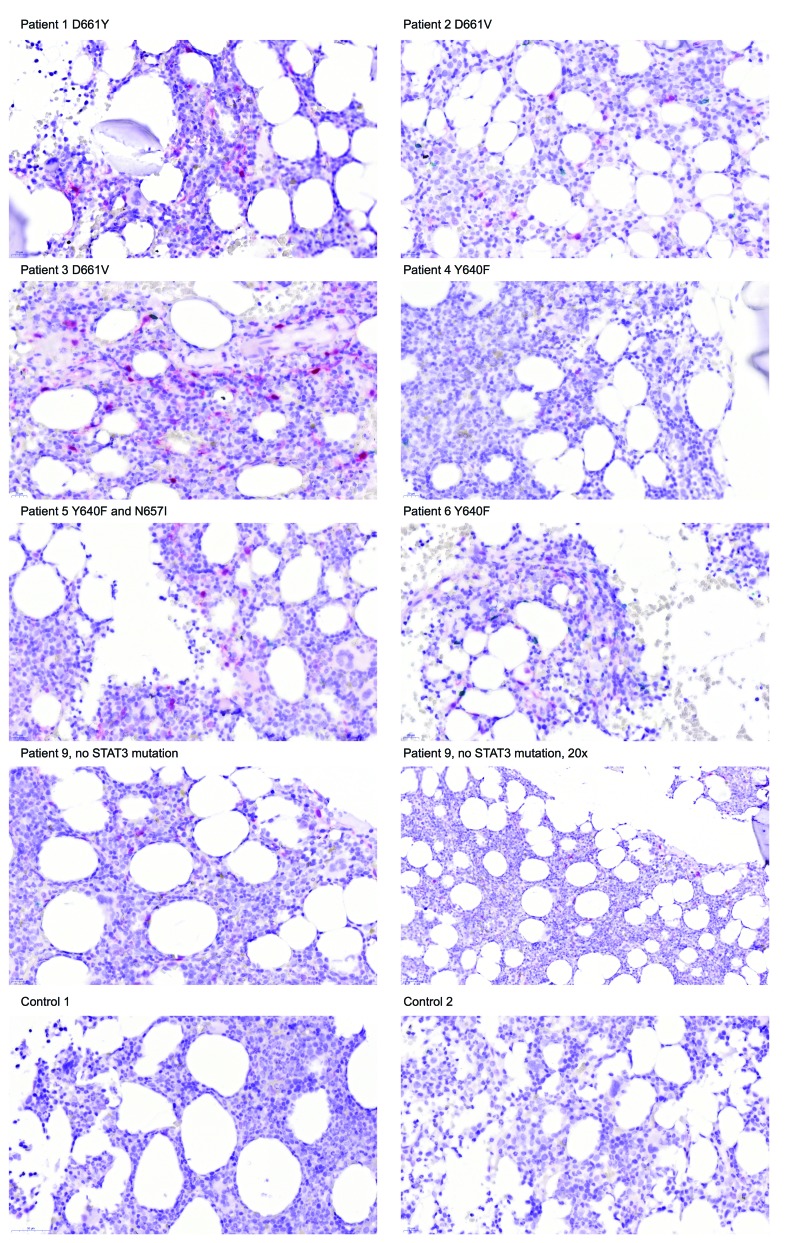
Felty syndrome is a rare disease defined by neutropenia, splenomegaly, and rheumatoid arthritis. Sometimes the differential diagnosis between Felty syndrome and large granular lymphocyte leukemia is problematic. Recently, somatic and mutations were discovered in 30-40% of patients with large granular lymphocyte leukemia. Herein, we aimed to study whether these mutations can also be detected in Felty syndrome, which would imply the existence of a common pathogenic mechanism between these two disease entities. We collected samples and clinical information from 14 Felty syndrome patients who were monitored at the rheumatology outpatient clinic for Felty syndrome. Somatic mutations were discovered in 43% (6/14) of Felty syndrome patients with deep amplicon sequencing targeting all exons. Mutations were located in the SH2 domain of , which is a known mutational hotspot. No mutations were found. In blood smears, overrepresentation of large granular lymphocytes was observed, and in the majority of cases the CD8 T-cell receptor repertoire was skewed when analyzed by flow cytometry. In bone marrow biopsies, an increased amount of phospho-STAT3 positive cells was discovered. Plasma cytokine profiling showed that ten of the 92 assayed cytokines were elevated both in Felty syndrome and large granular lymphocyte leukemia, and three of these cytokines were also increased in patients with uncomplicated rheumatoid arthritis. In conclusion, somatic mutations and STAT3 activation are as frequent in Felty syndrome as they are in large granular lymphocyte leukemia. Considering that the symptoms and treatment modalities are also similar, a unified reclassification of these two syndromes is warranted.
费尔蒂综合征是一种罕见疾病,其特征为中性粒细胞减少、脾肿大和类风湿关节炎。有时,费尔蒂综合征与大颗粒淋巴细胞白血病之间的鉴别诊断存在问题。最近,在 30-40%的大颗粒淋巴细胞白血病患者中发现了体细胞 和 突变。在此,我们旨在研究这些突变是否也能在费尔蒂综合征中检测到,如果可以,则意味着这两种疾病实体之间存在共同的致病机制。我们收集了 14 名在风湿免疫科门诊监测费尔蒂综合征的费尔蒂综合征患者的样本和临床信息。通过靶向所有外显子的深度扩增子测序,在 43%(6/14)的费尔蒂综合征患者中发现了体细胞 突变。突变位于 的 SH2 结构域,这是一个已知的突变热点。未发现 突变。在血涂片上观察到大颗粒淋巴细胞的过度表达,并且在大多数情况下,通过流式细胞术分析时,CD8 T 细胞受体谱发生了偏倚。在骨髓活检中,发现了大量磷酸化 STAT3 阳性细胞。血浆细胞因子谱分析显示,在费尔蒂综合征和大颗粒淋巴细胞白血病中,有 10 种测定的细胞因子升高,其中 3 种细胞因子在单纯性类风湿关节炎患者中也升高。总之,体细胞 突变和 STAT3 激活在费尔蒂综合征和大颗粒淋巴细胞白血病中同样常见。鉴于症状和治疗方式也相似,有必要对这两种综合征进行统一的重新分类。